Introduction
Pulsed electromagnetic field (PEMF) therapies represent a non-invasive modality, approved by the FDA in 1979 for the treatment of non-union bone fractures [1]. Recently, a review suggested that the mechanisms underlying PEMF action justify its use as an adjuvant in exercise-based interventions, since electromagnetic stimulation appears to enhance cellular responses related to angiogenesis, mitochondrial biogenesis, and the activation of regenerative and muscle growth pathways [2, 3].
Preliminary studies, albeit often limited by small sample sizes and methodological constraints, suggest that the combination of PEMF and physical exercise may enhance both functional and morphological adaptations, as observed in acute and chronic contexts. However, these findings should be interpreted with caution due to the heterogeneity in PEMF parameters and study designs [4, 5]. Improvements in cardiovascular parameters and post-exercise recovery have also been observed in cycling ergometer protocols combined with magnetic stimulation [4]. In longer-term interventions involving clinical populations, such as patients with subacromial impingement syndrome, PEMF combined with exercise has demonstrated superior outcomes compared to placebo plus exercise, including improvements in muscle strength and functional capacity [6]. While these findings illustrate the therapeutic potential of PEMF in rehabilitation settings, direct extrapolation to healthy, untrained adults should be made with caution due to differences in baseline physiology and adaptation mechanisms. Complementarily, Kinney et al. [7] used magnetic resonance imaging to report a 15.4% increase in rectus abdominis thickness and an 18.6% reduction in subcutaneous abdominal fat after application of a combined high-intensity focused PEMF and radiofrequency (RF) device. While these findings suggest potential effects on muscle hypertrophy and tissue remodelling, the concomitant use of RF energy precludes isolating the specific contribution of PEMF to the observed adaptations. In older adults, a 12-week protocol with weekly PEMF exposure was associated with increased muscle strength and significant improvements in functional mobility tests such as the Timed Up and Go and Sit-to-Stand [8]. Additionally, some recent work has shown that PEMF is a potential promoter of modulations at the muscular morphological level and impacts muscular strength adaptations [9, 10].
These findings extend beyond functional and morphological responses. Animal models have shown that PEMF can modulate molecular pathways involved in skeletal muscle homeostasis (Akt/mTOR signalling) and responsible for promoting protein synthesis and inhibiting the FoxO1 pathway and the Myostatin/ActRIIB axis, both associated with muscle protein degradation [11–13]. Translating the certainty of these findings to humans, particularly in healthy untrained individuals, remains moderate and should be interpreted with caution due to interspecies differences and distinct physiological contexts. These responses have been documented in the contexts of immobilisation-induced atrophy, diabetes, and traumatic injury, where PEMF showed therapeutic potential by preserving muscle mass, promoting fibre hypertrophy, and increasing the activity of key metabolic enzymes such as succinate dehydrogenase and malate dehydrogenase. However, most of these findings come from studies with animals or clinical populations, which limits the extrapolation of results to healthy individuals. Although PEMF appears to share some physiological outcomes with traditional resistance training, such as improvements in muscle thickness, strength, and physical performance, evidence in healthy, untrained adults remains scarce and inconsistent, with some studies reporting negligible morphological effects [8, 9]. Therefore, its effectiveness in this population remains poorly established and warrants further investigation.
Adaptations such as increases in muscle thickness, maximal strength, and muscular endurance are essential attributes for musculoskeletal health and are typically associated with conventional resistance training protocols. Therefore, the present study aimed to evaluate the effects of an eight-week continuous PEMF application protocol, in comparison with conventional unilateral resistance training on a leg extension machine (EXT), on the thickness of the proximal (RF30%) and mid (RF50%) rectus femoris and mid vastus later-alis (VL50%) muscles. As secondary outcomes, changes in one-repetition maximum strength (1RM) and muscular endurance during knee extension at 60% of 1RM were also assessed. The EXT group served as a positive control. Additionally, individual responsiveness was analysed through responder/non-responder classification. Two hypotheses were tested: (H1) both protocols would increase muscle thickness at RF30%, RF50%, and VL50%; and (H2) both interventions would result in gains in 1RM strength and muscular endurance during knee extension.
Material and methods
Experimental approach
This study is characterised as a chronic, randomised, and parallel experimental trial conducted over an eight-week period during the year 2024 at a university located in the Central-West region of Goiás, Brazil. Participants were recruited by convenience sampling within the university through personal invitations made by the research team, as well as through informational postings in academic groups and on social media platforms. Prior to the start of the experimental protocol, all volunteers signed a written informed consent form, which provided detailed information about the procedures, as well as the potential risks and discomforts associated with participation. In addition to the written document, all procedures were explained verbally to the participants to ensure full understanding of the study’s scope and requirements.
Study design
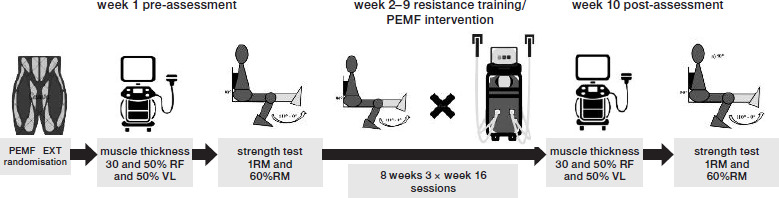
Participants were randomly allocated by draw into one of two experimental groups: PEMF or EXT. The protocol lasted a total of 10 weeks, with the first and final weeks dedicated to the assessment of primary and secondary outcome variables. Participants trained 3×/week for a maximum of 30 min/session. A total of 24 training sessions were completed by each group. The PEMF protocol was conducted in a temperature-controlled room, maintained between 21 and 23°C, while the EXT protocol was performed in a gym environment with ambient temperatures ranging from 23 to 26°C. The study design is illustrated in Figure 1.
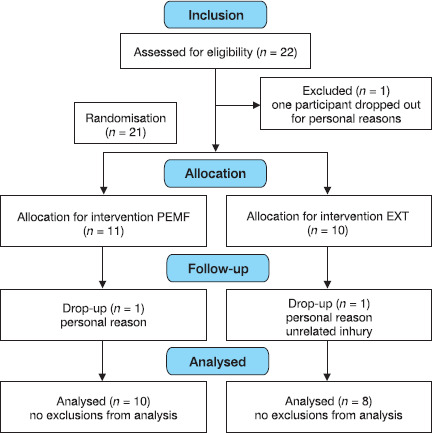
Participants
Untrained individuals of both sexes, aged between 18–35 years, were recruited for this study. Inclusion criteria required that participants had not engaged in any form of resistance training intervention within the previous six months, although individuals with prior familiarisation with such exercises were not excluded. Participants were also required to be healthy and free from any history of injuries to the hip, knee, or ankle joints. Exclusion criteria included the use of ergogenic supplements, a history of alcohol or tobacco use, and failure to attend at least 90% of the scheduled training sessions. During the recruitment phase, 22 participants met the eligibility criteria and were enrolled in the study. However, over the course of the intervention, four participants withdrew, resulting in a final sample of 18 participants (5 men and 13 women). Table 1 presents the demographic and anthropometric characteristics of the participants. Table 2 presents the performance characteristics of the participants.
Table 1
Demographic and anthropometric characteristics of participants
Table 2
Performance characteristics of participants
[i] PEMF – pulsed electromagnetic field, EXT – traditional resistance training (leg extension), RF30% R/L – proximal rectus femoris thickness (right/left), RF50% R/L – mid rectus femoris thickness (right/left), VL50% R/L – mid vastus lateralis thickness (right/left), 1RM R/L – one-repetition maximum (right/left), 60% 1R M R/L – muscular endurance at 60% 1R M (right/left). Normality was confirmed for all baseline variables, which are expressed as mean ± standard deviation * statistically significant difference between groups
Experimental PEMF intervention
For this study, we used the Supramaximus model SMX-01 (Adoxy™, Votorantim, SP, Brazil), a portable PEMF device approved for clinical use by the Brazilian Health Regulatory Agency (ANVISA). The device operates with adjustable frequencies from 1 to 100 Hz, delivers a biphasic pulsed waveform, and provides a maximum magnetic flux density of 7 teslas per applicator. The intensity can be modulated from 10% to 100% of maximum output. Technical specifications are provided in the manufacturer’s user manual and comply with IEC 60601-1 safety standards for electro-medical equipment. Although no peer-reviewed reliability study (ICC) is currently published for this specific device, its clinical validation is supported by prior pilot studies using the same equipment [8, 14] and by its regulatory approval for human use. The equipment includes four extendable applicators, two of which are concave and two flat. Each PEMF pad consisted of a pair of Helmholtz coils (15 cm × 15 cm) housed in an ergonomically contoured applicator. For the purposes of this study, the application parameters included: percentage output intensity (measured in magnetic flux density – teslas), stimulation frequency (Hz), and total stimulation time (seconds).
The electromagnetic stimuli were applied under two distinct conditions. The submaximal condition was characterised by a pulsed stimulation pattern with pulse intervals of less than one second, while the supra-maximal condition consisted of sustained tetanic contractions for a predetermined duration. The equipment delivered a maximum output of 7 teslas per applicator, with the stimulation intensity adjusted proportionally to this maximum. The PEMF intervention was performed 3×/week, on Mondays, Wednesdays, and Fridays, always at the same time of day, with a 48-hour interval between sessions. Each session had a fixed duration of 30 min, as used in previous studies with PEMF for morphological and functional adaptations [14]. The stimulus intensity was progressively increased each week, following the principle of progressive over- load and based on protocols established in the magnetic stimulation literature and manufacturer recommendations, in addition to ensuring participant adherence, during the procedure, participants remained seated close to the device. The applicators were positioned directly on both thighs, with their centres aligned with the midpoint between the anterior superior iliac spine and the superior border of the patella, ensuring coverage of the proximal to the middle portion of the quadriceps. The concave applicators were oriented longitudinally along the muscle belly and secured with adjustable elastic straps to prevent movement during stimulation, covering a significant portion of the rectus femoris (RF) and adjacent musculature, including the vastus lateralis (VL). The detailed configuration parameters used throughout the intervention sessions are presented in Table 3.
Table 3
PEMF intervention protocol
The definition of the parameters used in the PEMF protocol was based on experimental and clinical evidence supporting its efficacy in promoting muscular adaptations. The choice of a progressive intensity ranging from 20% to 100% (based on a maximum output of 7.0 teslas per applicator), applied in 30-minute sessions, three times per week for eight weeks, is supported by studies such as [7, 15, 16], which employed regular high-intensity applications in untrained or clinical populations. Figure 2 presents a schematic proposal for the application of PEMF. Technical information about the PEMF equipment is available in Table 4.
Table 4
Technical information for PEMF equipment (adoxy supramaximus)

Four applicators (two concave and two flat) were positioned on each thigh, with the concave applicators aligned over the RF and the lateral applicators placed proximally over the VL. Applicators were secured with adjustable elastic straps to prevent movement during stimulation.
Resistance training protocol
A parallel intervention group was allocated to perform unilateral knee extension training on a leg extension machine (EXT). Ultrasound assessments and strength testing were performed by assessors blinded to the group allocation, and the participants were instructed not to disclose their group assignment during the testing sessions. The unilateral design was chosen to allow finer load progression and to isolate quadriceps adaptation.
The protocol followed the same intervention period as the PEMF group, with sessions held three times per week on Mondays, Wednesdays, and Fridays, always at the same time of day. Training sessions were conducted individually in either the morning (6:00–9:00 a.m.) or afternoon (2:00–4:00 p.m.) periods to ensure exclusive interaction between the instructor and each participant. All sessions were supervised by a certified physical education professional specialised in strength and conditioning, who was blinded to the study outcomes. The training protocol consisted of three sets of unilateral knee extension exercises, using loads adjusted within a repetition zone of 8 to 12 maximum repetitions, with one-minute rest intervals between sets. The equipment used was a leg extension machine (Lion Fitness®), which operates via a plate-loading resistance system. Prior to the start of the study, the machine was disassembled for calibration, and it was verified that the first two plates weighed 5 kg each, while the remaining plates increased the resistance by 7 kg per increment.
During the exercise, participants were positioned with their backs fully supported by the padded back-rest, maintaining constant contact between the lumbar and gluteal regions and the bench. The side han- dles were firmly held to avoid compensatory movements. The foam pad was placed between the medial and lateral malleoli, allowing proper execution of the knee extension movement. To ensure proper biomechanical alignment, a visual line was drawn between the patellofemoral joint and the pulley axis of the machine, which allowed individualised adjustments at the ankle, knee, and back support points based on each participant’s anthropometric characteristics. Before the first working set, participants performed a specific warm-up on the same equipment, completing 8 to 10 repetitions with a light load corresponding to approximately 40– 50% of their estimated maximal load, followed by a one-minute rest.
For the working sets, participants performed 8 to 12 repetitions per set. If more than 12 repetitions were completed in the first set, the exercise was interrupted and the load was increased by 1 to 2 kg in the following set using external plates added to the machine. Conversely, if fewer than eight repetitions were performed, the load was reduced accordingly. All sets were executed to concentric failure. Movement cadence was standardised: 1–2 s for the concentric phase and 2 s for the eccentric phase, with no pause between phases. Participants received verbal encouragement from the instructor throughout the sets, but no physical assistance was provided to move the weight. The instructor remained close to the participant throughout the training session, monitoring the load progression, number of sets and repetitions, and rest intervals. All participants, regardless of group allocation, were instructed to refrain from performing any additional lower-body exercises during the study. However, upper-body resistance exercises were permitted.
A standardised complementary training program was prescribed by a specialised team, including multi-joint upper-body exercises such as bench press, triceps extension, dumbbell shoulder press, lat pulldown, and seated cable row. Participants were also instructed to maintain their usual lifestyle habits and to avoid introducing new confounding factors such as starting new sports activities, using dietary supplements, or making abrupt changes to their dietary patterns.
Procedures
Bioimpedance analysis
For sample characterisation, a standardised identification form was used to record sex, age, and body mass data. Additionally, body composition was assessed using the bioelectrical impedance method (Thera Science, São José dos Campos, SP, Brazil), following strict pre-test preparation criteria. These included: a minimum fasting period of four hours prior to the test; no strenuous physical activity within the 24 h preceding the assessment; bladder emptying within 30 min before the test; abstinence from alcohol consumption for at least 48 h prior; suspension of diuretic medication seven days before testing; and supine rest for 5 to 10 min immediately prior to the assessment. The bioimpedance procedure was applied uniformly across all participants to ensure methodological consistency throughout the study. This method made it possible to reliably estimate the body fat percentage (%), lean body mass (kg), muscle mass (kg), and total body water (L).
1RM and 60% 1RM protocol
The legs were tested unilaterally, with the limb selected randomly by draw. After a 48-hour interval, the contralateral leg was assessed following the same EXT procedure. The one-repetition maximum (1RM) determination protocol was conducted in advance and structured in sequential phases.
Initially, participants performed joint mobility exercises targeting the involved joint, followed by a specific warm-up on the leg extension machine simulating the unilateral knee extension movement. The first load attempt was set at approximately 50% of the participant’s self-estimated maximum, allowing for 6 to 8 repetitions, followed by a three-minute recovery interval. Next, the load was adjusted to 75% of the initial estimate, with 3 to 5 repetitions performed, followed by another three-minute rest period. After this preparatory phase, the first 1RM attempt was initiated. If the participant was able to perform more than one repetition, a five-minute rest was provided before a new attempt with a progressively increased load. Load increments were set at 7 kg whenever more than one repetition was completed. To increase the precision in determining the true maximal load, additional weight plates were attached externally to the machine’s weight stack, allowing for adjustments in 1, 2, 3, 4, or 5 kg increments. The 1RM protocol was applied in two separate sessions.
60% 1RM protocol
After completing the 1RM test, a passive rest period of 10 min was provided. During this interval, the load corresponding to 60% of the established 1RM was calculated. This working load was adjusted without informing the participant, in order to ensure blinding and avoid influencing performance during the test.
During the 60% 1RM test, participants were instructed to perform the maximum possible number of unilateral repetitions using the same leg extension equipment. To standardise execution, the concentric phase of the knee extension was performed in approximately 1 to 2 s, followed by the eccentric phase at the same cadence, with no pauses between movement transitions. Participant positioning was identical to that used during the 1RM test. The test was terminated when the participant attempted but could not complete an additional repetition. Verbal encouragement was permitted throughout the test; however, no external assistance was provided to help complete the repetitions.
Ultrasound measurements
Muscle thickness was assessed using B-mode ultrasound (Mindray M6, Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China) with a linear transducer (model L14-6Ns, frequency range: 6–14 MHz, footprint: 4.0 cm). The probe was placed perpendicular to the skin with minimal pressure to avoid tissue compression. A single image was obtained at each anatomical site. If the image quality was compromised (poor definition of muscle aponeuroses or distortion), a second image was acquired during the same session. RF muscle thickness was evaluated at two distinct points on the thigh, corresponding to 30% and 50% of the total femur length, while VL thickness was measured at the 50% femur length mark. The anatomical landmarks used to define measurement sites were the greater trochanter and the lateral femoral epicondyle. An anthropometric measuring tape (Sanny®) was used to ensure standardised distance measurements between landmarks. All image acquisition and analysis procedures were performed by a single trained investigator to ensure methodological consistency and minimise inter-rater variability; the investigator was blinded to group allocation (PEMF vs. EXT) during both image acquisition and analysis. Participants were instructed not to disclose their intervention group during assessment sessions. During image acquisition, participants remained at rest for 10 min, lying in a supine position on an examination table in a temperature-controlled room (21°C). The lower limbs remained relaxed throughout the procedure. After precise identification and marking of the measurement points, a generous amount of water-based ultrasound gel was applied to the skin and to the transducer tip to optimise the image quality. Care was taken to avoid excessive compression of the muscle tissue by the probe, which could compromise measurement accuracy. To ensure postural stability and minimise artifacts caused by involuntary movement, participants were instructed to remain completely still during the examination.
It is noteworthy that the execution and analysis of all ultrasound images were performed by the same investigator who led the methodological reliability study recently published by our group [17], involving a sample of 106 healthy individuals. That study demonstrated excellent intra-rater reliability (ICC = 0.998; MDD 0.074–0.082 cm), inter-rater reliability (ICC = 0.976– 0.977; MDD 0.269–0.270 cm), and inter-day reliability (ICC = 0.972–0.973; MDD 0.286–0.291 cm), even when accounting for sex and age subgroups.
In this context, the ultrasound protocol adopted in the present study is supported by robust reliability evidence obtained under identical acquisition conditions. In the validation study by Stausholm et al. [17] single-image measurements of rectus femoris thickness demonstrated excellent reproducibility. The intra-rater reliability for both raters was extremely high (ICC = 0.998 at both visits), with minimal detectable differences (MDDs: 0.074–0.082 cm). The inter-rater reliability was also excellent (ICC = 0.976 at visit 1 and 0.977 at visit 2; MDDs: 0.269–0.270 cm). The inter-day reliability remained comparably strong (ICC = 0.973 for rater A and 0.972 for rater B; MDDs: 0.286– 0.291 cm). Sensitivity analyses adjusting for age, sex, and the use of averaged versus single measurements yielded similar results, and no heteroscedasticity was observed. Together, these findings indicate that single-image acquisition – when performed using a rigorously standardised protocol – provides highly stable estimates of muscle thickness, with measurement error far below the magnitude of changes expected in longitudinal training studies.
Randomisation and allocation procedures
Participant randomisation was conducted in multiple stages by a researcher not involved in participant recruitment, assessment, or intervention delivery. The first stage involved a simple random draw to determine which leg would be used for the initial 1RM strength testing. The second stage-involved allocation into one of the two experimental groups (PEMF or EXT) using sequentially numbered, opaque, sealed envelopes prepared in advance. Each envelope contained a card indicating the group assignment, and envelopes were opened only after the participant had completed baseline assessments and signed the informed consent form. This procedure ensured allocation concealment and minimised selection bias. To control for the potential influence of lower-limb dominance on the results, participants were asked which leg they would use to kick a soccer ball, identifying their dominant leg. This information was used to ensure that no systematic preference for one limb was present during the group allocation.
Sample size calculation
The sample size was determined based on the following parameters: test family = F tests; statistical test = ANOVA repeated measures, within-between interaction; type of analysis = a priori computation required sample size. The input parameters for the analysis were: effect size = 0.40; alpha = 0.05; power = 0.85; number of groups = 2; number of measurements = 2, resulting in a total required sample of 18 participants. The choice of a large effect size (f = 0.40) was based on the magnitude of change observed in our prior feasibility study with PEMF [18], with this sample size (n = 18), the study was adequately powered (85%) to detect large interaction effects but may be underpowered to detect smaller, yet clinically meaningful, differences.
Statistical analysis
Data distribution and normality were assessed using the Shapiro–Wilk test. Baseline analytical data and primary outcomes were presented as mean and standard deviation (SD), while secondary outcomes were expressed as median and 95% confidence intervals (95% CI). Repeated measures ANOVA was used to compare muscle thickness values (RF30%, RF50%, and VL50% for both legs). The Wilcoxon signed-rank test was used to analyse changes over time for 1RM and 60% 1RM. Between-group comparisons for the same variables were performed using the Mann–Whitney U test. For ANOVA models, partial eta-squared ( 2p) is reported as the measure of effect size. For non-parametric comparisons (Wilcoxon and Mann–Whitney U tests), the effect size r (r = |Z|/N) is reported and interpreted as small (0.1), medium (0.3), or large (0.5). A significance level of p < 0.05 was adopted. All statistical analyses were performed using the IBM SPSS software, version 25. Graphical analyses were conducted using GraphPad Prism (version 8).
Results
Demographic and anthropometric variables were tested for Gaussian distribution. Normality was confirmed for all variables. The distribution behaviour of the primary dependent variables, muscle thickness at RF30%, RF50%, VL50%, and 1RM in both legs, was thoroughly assessed. Table 5 presents whether the normality assumptions for the muscle thickness variables were violated or preserved. Table 6 presents the normality status for the dependent variables related to strength and muscular endurance.
Table 5
Normality analysis of dependent variables: muscle thickness
Table 6
Normality analysis of dependent variables: 1RM and 60% 1RM
For the data analysis process, comparisons of demographic and anthropometric variables followed parametric assumptions and were conducted using independent t-tests. For the dependent variables related to muscle thickness, since the majority of the data did not violate normality assumptions, these variables were analysed parametrically using a 2 × 2 repeated measures ANOVA. Conversely, because most strength-related variables violated normality, 1RM and 60% 1RM were analysed using non-parametric methods: Wilcoxon signed-rank test for within-group (temporal) comparisons and the Mann–Whitney U test for between-group comparisons. For secondary outcomes (1RM and 60%1RM), multiplicity arising from segmented non-parametric testing was addressed by controlling the false discovery rate using the Benjamini–Hochberg adjustment (q = 0.05). These variables were presented as medians with 95% CI. Table 1 presents the morphological and performance characteristics of the participants. Comparisons between the intervention groups (PEMF and EXT) were performed using an independent samples t-test, indicating baseline equivalence between groups for the primary and secondary dependent variables. Figure 3 illustrates the participant inclusion and exclusion process.
Muscle thickness analyses
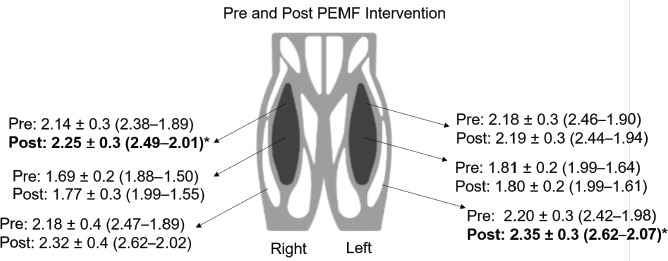
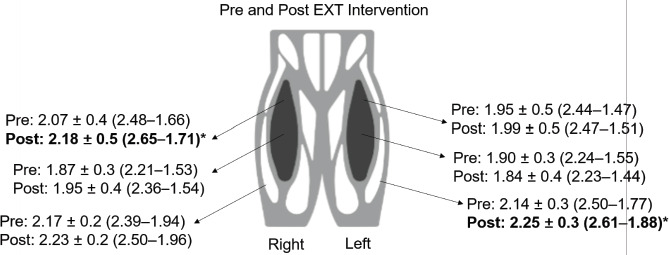
Repeated measures ANOVA revealed a significant time effect for right RF30% thickness (F1,16 = 9.976; p = p-values < 0.05 indicate a violation of normality * violation of normality 0.006; 2p = 0.384), but no significant group effect (p =0.570) or group × time interaction (F1,16 = 0.295; p = 0.594; 2p = 0.018). For right RF50%, no significant differences were observed for the time effect (F1,16 = 3.258; p = 0.090;2p = 0.169), group effect (p = 0.247), or group × time interaction (F1,16 = 0.174; p = 0.683; 2p = 0.011). Similarly, for VL50%, there were no significant differences for the time effect (F1,16 = 4.063; p = 0.061;2p = 0.203), group effect (p = 0.741), or group × time interaction (F1,16 = 0.768; p = 0.394;2p = 0.046).
No significant changes were observed for left RF30% muscle thickness with respect to the time effect (F1,16 = 0.356; p = 0.559; η 2p = 0.022), group effect (p = 0.411), or group × time interaction (F1,16 = 0.151; p = 0.703; η 2p = 0.009). The same was true for left RF50% regarding the time effect (F1,16 = 1.961; p = 0.180; η 2p = 0.109), group effect (p = 0.491), and interaction (F1,16 = 0.657; p = 0.429; η2p = 0.039). However, for left VL50%, a significant time effect was observed (F1,16 = 10.823; p = 0.005; η 2p = 0.404), with no significant group effect (p = 0.526) or group × time interaction (F1,16 = 0.012; p = 0.913;η2p = 0.001). Detailed pre- and post-intervention comparisons for the PEMF and EXT groups are presented in Figures 4 and 5, respectively.
Responders and non-responders to the PEMF and EXT interventions for muscle thickness
Participants were classified as responders only when individual changes in muscle thickness exceeded the site-specific minimum detectable difference, thereby accounting for ultrasound measurement error. For the RF30% measurement in the right leg, 80% of participants (n = 8) responded positively to the PEMF intervention, showing an average increase in muscle thickness of 7.7%. For the same measurement in the left leg, only 60% of participants (n = 6) responded to the intervention, with an average gain of 6.5%. Regarding the RF50% measurement in the right leg, only 50% of participants (n = 5) showed a positive response, with an average gain of 12.8%. However, for the left leg, only 40% (n = 4) responded positively to the PEMF intervention, with an average improvement of 5.2%. Lastly, for the VL50% measurement in the right leg, 70% (n = 7) responded positively, presenting an average gain of 9.7%, whereas in the left leg, 80% showed a positive response to the PEMF therapy, with an average increase of 10.8%.
In the context of the EXT intervention, for the RF30% measurement in the right leg, 75% of participants (n = 6) showed positive outcomes, with an average gain of 6.2%. For the same measurement in the left leg, only 50% of participants (n = 4) responded positively to the intervention, with an average increase of 8.3%. Regarding the RF50% measurement in the right leg, similarly, 75% of participants (n = 6) responded positively to the EXT intervention, presenting an average improvement of 5.7%. In the left leg, the gains were more modest (4.1%), with only 37.5% of participants (n = 3) showing a favourable response. Finally, for the VL50% measurement in the right leg, only 50% (n = 4) responded to the intervention, with an average increase of 7.5%. In contrast, for the left leg, 75% of participants (n = 6) responded positively to the EXT intervention, with an average gain of 8.7% in muscle thickness. Figure 6 presents the responders and non-responders to the PEMF and EXT interventions in terms of muscle thickness gains.
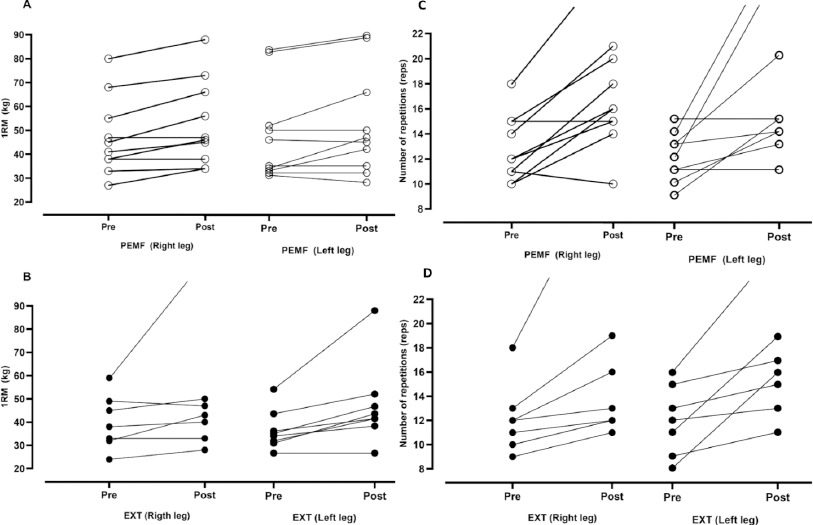
Figure 6
Responders and non-responders for 1RM across both interventions. Panel A shows data from the PEMF group, while panel B presents data from the EXT group. Responders and non-responders for 60% RM can be viewed in panels C and D. Panel C shows data from the PEMF group, while panel D presents data from the EXT group.
1RM analyses
The Wilcoxon signed-rank test was used to compare pre- and post-intervention medians in the PEMF group, showing significant improvements in unilateral knee extension strength for the right leg (Z = –2.527; p = 0.012, r = 0.80) and the left leg (Z = –2.103; p = 0.035, r = 0.67). Similarly, the EXT group exhibited significant gains in 1RM for the right leg (Z = –2.120; p = 0.034, r = 0.75) and the left leg (Z = –2.366; p = 0.018, r = 0.84). The Mann–Whitney U test revealed no significant differences between groups in the right leg 1RM at baseline (U = 31.500; Z = –0.759; p = 0.448, r = 0.18) or post-intervention (U = 33.500; Z = –0.578; p = 0.573, r = 0.14). The same was observed for the left leg at baseline (U = 23.500; Z = –1.470; p = 0.142, r = 0.35) and post-intervention (U = 31.500; Z = –0.757; p = 0.449, r = 0.18).
To account for multiplicity arising from segmented non-parametric testing, p-values were adjusted using the Benjamini–Hochberg false discovery rate procedure (q = 0.05). After Benjamini–Hochberg adjustment, significant within-group improvements in unilateral knee extension 1RM were observed in both intervention groups. In the PEMF group, 1RM increased significantly in the right leg (p adjusted = 0.024) and left leg (p adjusted = 0.035). Similarly, the EXT group demonstrated significant gains in 1RM for the right leg (p adjusted = 0.035) and the left leg (p adjusted = 0.024).
Between-group comparisons using the Mann–Whitney U test revealed no significant differences between the PEMF and EXT groups for 1RM at baseline or post-intervention (all p > 0.14). The results are presented in Table 7.
Table 7
1RM and 60% 1RM repetitions before and after intervention
60% 1RM repetition analysis
For the PEMF group, the Wilcoxon test showed significant improvements in the number of repetitions completed at 60% 1RM for the right leg (Z = –2.552; p = 0.011; r = 0.81) and the left leg (Z = –2.366; p = 0.018; r = 0.75). Similar results were observed in the EXT group for the right leg (Z = –2.536; p = 0.011; r = 0.90) and the left leg (Z = –2.536; p = 0.011; r = 0.90). The Mann–Whitney U test showed no significant between-group differences in the pre-intervention condition for 60% 1RM of the right leg (U = 30.500; Z = –1.470; p = 0.392; r = 0.20) or for the left leg (U = 38.000; Z = –0.856; p = 0.858; r = 0.10).
To ensure that we are not incurring a type 2 error, we apply the same stiffness of adjustment. Regarding muscular endurance, assessed as repetitions performed at 60% of 1RM, both groups exhibited significant improvements following Benjamini–Hochberg correction. In the PEMF group, the number of repetitions increased significantly for the right leg (p adjusted = 0.024) and the left leg (p adjusted = 0.024). Comparable improvements were observed in the EXT group for both the right leg (p adjusted = 0.024) and the left leg (p adjusted = 0.024).
Between-group comparisons using the Mann–Whitney U test revealed no significant differences between the PEMF and EXT groups for 60% 1RM at baseline or post-intervention (all p > 0.14). The results are presented in Table 7.
Responders and non-responders to the PEMF and EXT interventions for 1RM and 60% 1RM
Regarding PEMF, 70% (n = 7) of the sample responded positively to the intervention for 1RM on the right leg, showing an increase in the maximum load lifted. The average magnitude of load increase among responders was 15%. In contrast, for the left leg, only 50% (n = 5) showed an increase for 1RM (the average magnitude among responders was 21%). For the EXT intervention, 75% (n = 6) of the participants exhibited a positive response for the 1RM on the right leg. Participants showed a reasonably higher average increase magnitude (24%). For the left leg, 87.5% (n = 7) exhibited a positive response for the 1RM, and the same occurred for the magnitude of the gains, showing a 30% improvement after the intervention.
In the context of performance at 60% 1RM, 80% (n = 8) of participants responded positively to the PEMF intervention, demonstrating an improvement in the number of repetitions performed with the right leg, with an average increase of 55% from pre- to post-intervention. Similarly, for the left leg, PEMF elicited a positive response in 80% (n = 8) of the participants, with an average increase of 61% in the number of repetitions. Lastly, following the EXT intervention, 100% (n = 8) of participants improved strength endurance performance in the right leg, with the same proportion observed for the left leg (100%; n = 8). Nevertheless, the magnitude of improvement in the number of reps was comparatively more modest: 29% for the right leg and 48% for the left leg. Figure 4 A–D illustrates the individual responses of participants classified as responders and non-responders to the PEMF and EXT interventions.
Adverse effects of PEMF treatment
Adverse effects associated with the PEMF intervention were monitored throughout all sessions, which followed a fixed schedule and standardised applicator positioning protocol, consistent with the principle of progressive overload typically used in resistance training. Perceived exertion and potential discomfort were monitored in all sessions using an adapted Borg scale from 0 to 10, as employed in our previous pilot study [9]. Participants rated their sensation immediately after each session, and any score 6 (moderate discomfort) prompted further investigation to detect possible adverse effects. During the initial sessions, the intensity of the magnetic flux was set at lower levels (25–30% flux density), with gradual increments applied throughout the intervention. This approach facilitated participant adaptation and enhanced adherence to the treatment. No adverse effects were reported during the study, including no localised increase in skin temperature, itching, pain, or other discomforts commonly associated with electrical stimulation-based therapies.
Discussion
The present study aimed to investigate the effects of a continuous PEMF stimulation protocol on muscle thickness and strength performance in untrained individuals, in comparison with a traditional resistance training protocol (EXT). Changes in the thickness of the RF30% and RF50% portions of the rectus femoris muscle, as well as the VL50% portion of the vastus lateralis, were analysed, in addition to strength gains assessed through one-repetition maximum (1RM) and muscular endurance (60% 1RM) in the knee extension exercise. To our knowledge, this is one of the first studies to evaluate structural and functional adaptations induced by PEMF in an ecologically valid training context, using ultrasonographic measurements and direct comparison with traditional resistance training, providing promising preliminary data on its effectiveness as a standalone intervention strategy.
The primary hypothesis (H1), which posited that both protocols would lead to a significant increase in muscle thickness at RF30%, RF50%, and VL50%, was partially confirmed, as only the right leg RF30% and the left leg VL50% showed significant effects. The lack of consistent hypertrophy across all measured sites may be attributed to several interrelated factors: (1) the 8-week intervention period may have been insufficient for PEMF to induce detectable morphological changes in untrained muscle; (2) PEMF may prioritise neural adaptations (as reflected in strength gains) before structural hypertrophy; (3) the selected PEMF parameters (intensity, frequency) might represent a suboptimal dose for maximising hypertrophic responses; and (4) ultrasound-based thickness measurements, while valid, may lack the sensitivity to detect subtle changes in early-stage adaptations. In contrast, the secondary hypothesis (H2) was supported, given that both groups exhibited significant improvements in maximal strength and muscular endurance performance in both legs. These findings support the feasibility of applying PEMF, which is capable of eliciting relevant morphofunctional adaptations even in the absence of mechanical overload [15].
One of the first studies to examine the effects of PEMF intervention on muscle mass was conducted by Duncan and Dinev [13], who reported significant increases in muscle fibre density by 20.56% in an animal model. While such mechanistic findings provide biological plausibility for PEMF-induced hypertrophy, direct extrapolation to humans requires caution due to interspecies differences in physiology, dosing, and adaptive responses. In humans, the available evidence remains relatively scarce. However, the increase in muscle thickness observed in our study is consistent with previous evidence. Kinney et al. [7] reported a 15.4% increase in rectus abdominis thickness after eight weeks of high-intensity PEMF application, with no changes in diet or body mass. Two months after the intervention, there was also an 18.6% reduction in adi-pose tissue thickness, accompanied by a 10.4% reduction in rectus abdominis diastasis. These changes were not associated with alterations in diet or body weight among participants, suggesting that the effects were directly attributable to the PEMF treatment. These findings are also reported in the study by Venugobal et al. [8]. The literature suggests that PEMF can modulate pathways involved in protein synthesis (such as the Akt/mTOR cascade), satellite cell activation, and muscle angiogenesis [19, 20].
Although this study did not directly investigate the molecular mechanisms involved, the literature provides a consistent body of evidence that allows for the inference of potential physiological pathways mediated by PEMF application. In vitro studies and animal models indicate that pulsed electromagnetic stimulation can induce direct depolarisation of peripheral motor neurons, leading to intense and repeated muscle contractions. This activation results in the release of acetylcholine at the neuromuscular junction, subsequently opening voltage-gated calcium channels, increasing intracellular Ca2+ levels, and triggering the contractile process even in the absence of voluntary stimulation [19, 20].
In addition to the neurophysiological effects, PEMF also appears to directly modulate molecular pathways involved in the regulation of muscle growth and maintenance. Some studies have demonstrated that exposure to PEMF activates intracellular cascades such as PI3K/Akt/mTOR, promoting protein synthesis and muscle hypertrophy [3, 21]. In parallel, the inhibition of catabolic factors such as FOXO1 and the Myostatin/ActRIIB axis has also been observed, both of which are frequently associated with protein degradation and muscle atrophy, particularly under conditions of immobilisation or chronic disease. Another relevant aspect concerns angiogenesis and tissue regeneration [22]. Studies conducted in animal models have reported increased capillary density and elevated expression of factors such as VEGF (vascular endothelial growth factor) following PEMF application, indicating the promotion of an environment conducive to muscle perfusion and local metabolic support [23]. This adaptation may partly explain the gains observed in both muscular endurance and functional recovery reported in clinical investigations [18, 24].
In the energetic context, the stimulation of oxidative metabolism induced by electromagnetic exposure also emerges as a potential mechanism for improving fatigue tolerance. The activation of pathways related to mitochondrial biogenesis, such as PGC-1 , as well as the modulation of oxidative enzymes, appears to occur in response to PEMF intervention [25, 26]. These effects may help explain, albeit indirectly, the improvement in repetitive performance under submaximal loads observed in the present study. Taken together, these mechanisms support the hypothesis that PEMF acts through complementary and potentially synergistic pathways to resistance training, thereby justifying the outcomes observed even in untrained individuals over a short intervention period.
Our study employed ultrasound-based measurements, a well-validated method for assessing muscle morphology, to detect structural modifications induced by PEMF in comparison with traditional training. In this context, the ultrasound protocol adopted in the present study is supported by robust reliability evidence obtained under identical acquisition conditions. In the reliability study by Stausholm et al. [17], single-image measurements of rectus femoris thickness demonstrated extremely high intra-rater reliability (ICC = 0.998 at both visits), with minimal detectable differences (MDDs: 0.074–0.082 cm). The inter-rater reliability was also excellent (ICC = 0.976 at visit 1 and 0.977 at visit 2; MDDs: 0.269–0.270 cm). The inter-day reliability remained comparably strong (ICC = 0.973 for rater A and 0.972 for rater B; MDDs: 0.286–0.291 cm). Sensitivity analyses adjusting for age, sex, and the use of averaged versus single measurements yielded similar results, and no heteroscedasticity was observed.
We also need to highlight that ultrasound measurement is a unidimensional technique, which may render it less sensitive to subtle variations, thereby hindering the detection of statistically significant changes in response to small modifications [27]. Soares et al. [28], in a recent meta-analysis, reported average variations between 0.27 and 0.29 cm in quadriceps muscles following resistance training. In our study, the changes were more modest (PEMF: 0.15 cm; EXT: 0.11 cm in VL50%), which may be attributed to methodological differences and the participants’ initial level of deconditioning. Enes et al. [29] also emphasised that changes in muscle thickness may not reach statistical significance, even in the presence of relevant physiological effects, particularly in short-term interventions.
Regarding the analysis of responders and non-responders in muscle thickness outcomes, our findings support a growing body of evidence highlighting substantial interindividual variability in hypertrophic adaptations, both in PEMF and traditional resistance training interventions. In total, 55.5% of participants in the PEMF group and 50% in the EXT group were classified as responders in at least one muscle thickness measure, while 44.5% (PEMF) and 50% (EXT) showed no detectable changes beyond the technical error of measurement. This heterogeneity may be attributed to intrinsic biological factors, such as genetic profile, anabolic sensitivity, or hormone status, as well as extrinsic factors, including measurement sensitivity, measurement error (SEM, MDD), intervention duration, or the specificity of the protocol. Pickering and Kiely [30] emphasise that the term ‘non-responder’ should be interpreted with caution, as the absence of adaptation may reflect suboptimal stimulus dosing rather than true inefficacy. Our findings are also consistent with those of Nunes et al. [31], who demonstrated marked variability in hypertrophic responses across different regions of the same muscle, suggesting that training adaptations are highly localised and do not follow a uniform growth pattern. Additionally, our analysis aligns with the methodological principles proposed by Chaves et al. [32], who advocate for within-individual experimental designs to isolate true training-induced responses, separating them from biological noise and measurement error.
The results related to strength performance revealed that both the PEMF protocol and traditional resistance training (EXT) were effective in promoting significant gains in 1RM and muscular endurance. The improvement in maximal strength performance observed in the PEMF group is particularly noteworthy, as it represents a protocol free from mechanical overload and with potential applicability in populations with reduced physical and functional capacity.
These findings suggest that PEMF is capable of triggering neuromuscular adaptations similar to those induced by conventional resistance exercise. Such adaptations may reflect, at least in part, neural mechanisms, which is consistent with the well-established principle that early strength gains in untrained individuals are predominantly neural in origin [33], including increased motor unit recruitment, enhanced inter- and intramuscular synchronisation, reduced antagonist co-activation, and greater efficiency in cortical and spinal activation [30, 34]. It is clear that the stimulation promoted by PEMF appears to act directly on peripheral motor neurons, without directly involving voluntary muscle contraction. However, afferent feedback at various levels does not exempt the central nervous system from its regulatory functions and adaptive responses [35]. In one of the few studies presented in the literature, Leonardo et al. [18] demonstrated a 27% improvement in knee extension strength in sarcopenic older adults following a PEMF intervention. However, maximal isometric knee extension strength cannot be directly compared to the dynamic strength exerted during a 1RM test.
The positive effect on muscular endurance, assessed through the number of repetitions performed at 60% of 1RM, also reinforces the functional efficacy of PEMF. Campos et al. [36] demonstrated that sessions involving greater contractile volume, even under moderate loads, promote adaptations in local muscular endurance. In the PEMF group, the repeated exposure to tetanic contractions during the 30-minute sessions may have metabolically simulated an environment similar to that of high-repetition sets, thereby fostering adaptations related to energy efficiency and fatigue tolerance. Although we did not directly assess metabolic or vascular parameters, in vitro studies and animal models suggest that PEMF can regulate intracellular calcium levels, activate AMPK-related pathways, and promote mitochondrial biogenesis and local vascularisation [3, 19], mechanisms that could underlie the endurance improvements observed here.
Our data indicated that more than three-quarters of the participants exceeded the minimum detectable change (MDC) thresholds derived from measurement error. Although the absence of a sham control group limits the causal attribution of these responses exclusively to PEMF, exceeding the MDC suggests that the observed changes are likely not solely due to technical variability or spontaneous fluctuation, in addition to the findings corroborating the effectiveness of both interventions in improving maximum strength (1RM) and muscular endurance (60% of 1RM). Individual-level analysis showed that 77.7% of participants in the PEMF group and 75% in the EXT group were classified as responders in at least one of the strength assessments. Dankel and Loenneke [37] emphasise that the classification of responders should be based on statistically exceeding the limits of random error, which requires not only pre- and post-intervention comparisons but also the inclusion of time-matched control groups capable of isolating true physiological responses from biological and statistical noise. The absence of a response in certain variables, such as muscle strength, may reflect limitations in stimulus dosage as well as interindividual differences modulated by genetic, metabolic or hormonal factors, or even baseline molecular pathway activity [38]. Therefore, the non-responsiveness observed in a minority of participants should not be interpreted exclusively as a protocol failure but rather as a reflection of the adaptive complexity to exercise.
Limitations
The primary limitation of this study is its modest sample size. Although an a priori calculation indicated the study was adequately powered (85%) to detect large effect sizes (f = 0.40) based on prior pilot data, the final sample (N = 18) inherently limits the statistical power to detect smaller, yet potentially clinically relevant, between-group differences. A post-hoc sensitivity analysis indicated that the study had 80% power to detect a difference in muscle thickness change of approximately 0.30 cm, aligning with a clinically relevant threshold. However, more subtle effects may have gone undetected (type II error), and the precision of our effect estimates is reduced. Consequently, the findings should be interpreted as preliminary estimates of effect, and their generalisability is constrained.
An important methodological consideration of the present trial is its parallel, non-controlled design, which limits internal validity and the causal attribution of the observed effects to PEMF per se. Although the EXT group functioned as an active comparator, the absence of a sham PEMF or time-matched no-treatment control prevents the dissociation of true physiological adaptations from expectancy-related influences, differential motivation during post-testing, and repeated-testing effects, particularly for outcomes such as 1RM and repetition-to-fatigue, which are known to be sensitive to learning and familiarisation. While exceeding the minimum detectable change supports that the observed responses likely surpassed random measurement error, this statistical threshold does not eliminate potential bias arising from non-specific effects. Therefore, the present findings should be interpreted as preliminary and hypothesis-generating, reinforcing the need for future trials employing rigorous sham-controlled or crossover designs to isolate the specific contribution of PEMF to neuromuscular adaptations.
Another limitation was the significant baseline difference in body fat percentage between groups (EXT: 30.1 ± 7.3%; PEMF: 22.8 ± 5.8%; p < 0.05), which likely reflects the unequal distribution of female participants (PEMF: 3 men/7 women; EXT: 2 men/6 women). However, body fat percentage is unlikely to have substantially confounded the primary outcomes of muscle thickness or strength adaptations in response to the specific interventions employed.
Participant and intervention-provider blinding was not feasible due to the fundamentally different nature of the PEMF and resistance training protocols; however, the outcome assessors were blinded and strict allocation concealment procedures were implemented to minimise detection and measurement bias.
Finally, another noteworthy limitation is the lack of rigorous dietary control during the intervention period, which may have introduced variability in the results related to body composition and performance [39]. Furthermore, the sample consisted exclusively of young, untrained individuals, making it inappropriate to extrapolate the observed effects to active populations, athletes, or individuals with chronic diseases.
Conclusions
The present study offers preliminary evidence that continuous PEMF application, even in the absence of mechanical overload, can elicit improvements in muscle morphology, maximal strength, and muscular endurance in untrained individuals. However, because the trial was not designed or powered to test equivalence or non-inferiority relative to resistance training, these findings should be interpreted cautiously. Given the modest sample size, the results are best viewed as early indications that PEMF may induce meaningful adaptive responses, underscoring the need for larger, rigorously controlled studies to confirm these effects and determine their comparative efficacy.