Introduction
Paralympic Powerlifting (PP) is an adapted sport that has been part of the Olympic circle for more than 45 years and is now practiced in almost 100 countries [1]. PP practice challenges the maximal upper limb strength of athletes with physical impairments such as lower limb amputations or malformations, spinal cord injuries, short stature, ataxia, and others [2]. During competition, athletes separated by body-weight categories have three attempts to lift the heaviest weight possible in the adapted bench press, with strictly technical judgement by PP referees, as intended in the PP rules and regulations [3]. Importantly, PP practice and competition depend not only on physical and technical factors but also on psychological factors [4, 5].
Several psychological factors can affect an athlete’s performance during competitions. Some of those are the different forms of anxiety. State anxiety refers to a temporal condition that can arise in response to stressful events such as competitions. In this sport-specific context, state anxiety is known as pre-competitive anxiety [6]. Depending on its magnitude, pre-competitive anxiety can be a facilitating stimulus that can maintain the athlete’s focus to achieve higher performance. However, if the anxiety levels are too high, it can be detrimental to their performance [7]. In addition, athletes can have a predisposition to experience higher levels of anxiety. Trait anxiety is a personality trait that increases the anxiogenic response to stressful situations, causing the athlete to feel higher anxiety levels than could normally be perceived [6].
Other important psychological factors that interfere with competitive performance are mood states. Mood states can predict, to some extent, the athlete’s success in a competition. While mood profiles higher in vigour can indicate good competitive performance, the predominance of negative mood dimensions, such as confusion, tension, anger, fatigue, and depression, is all related to poor sports performance [8–10]. In addition, depression is also a mental disorder that can significantly interfere with sport performance as it is related to reduced concentration, fatigue, disturbed sleep, and poor motivation [11]. Taken together, mental health determinants like trait anxiety, depression, and negative mood states can affect the well-being and quality of life of an athlete and consequently impair their competitive success [12].
Research on able-bodied athletes’ mental health indicates that differences can be found between men and women. Evidence shows that female athletes report higher anxiety, depression, and distress than males, while males report higher alcohol, drug, and gambling abuse [13]. There is a need to undertake research into the mental health of athletes with disabilities participating in para-sport, since reviews on the subject are inconclusive due to the lack of studies assessing this population [14]. Within this context, studies evaluating differences in psychological factors between male and female para-athletes are also scarce. Therefore, it is still unknown how psychological factors can vary between male and female para-powerlifters.
This study aims to compare pre-competitive anxiety, trait-state anxiety, mood state, depression, and quality of life measures between male and female athletes before a national-level Paralympic Powerlifting competition.
Material and methods
Sample
The sample consisted of 41 PP athletes, comprising 26 males (33.88 ± 11.16 years) and 15 females (32.13 ± 10.65 years). The sample’s competitive level included national and international-level athletes. The inclusion criterion was to have participated in the competition and completed it without having been disqualified for any reason.
Instruments
Pre-competitive anxiety
The pre-competitive anxiety of the athletes was measured with the Competitive State Anxiety Inventory Questionnaire-II (CSAI-2), translated and validated by Fernandes et al. [15]. This questionnaire is composed of 27 items divided into 3 subscales: cognitive anxiety, somatic anxiety, and self-confidence. The response scale for all items ranged from 1 to 4: 1 = nothing, 2 = something, 3 = moderate, and 4 = great. According to Alejo et al. [16], the score of each subscale was obtained by summing the scores of its corresponding items. The cognitive anxiety subscale included items 1, 7, 10, 13, 16, 19, 22, and 25, the somatic anxiety subscale included items 2, 5, 8, 11, 14, 17, 20, 23, and 26, and the self-confidence subscale included items 3, 4, 6, 9, 12, 15, 18, 21, 24, and 27. The resulting subscale scores were interpreted as follows: low (9 to 18 points), average (19 to 27 points), or high (28 to 36 points) [16].
Trait-state anxiety
Trait-state anxiety was measured with the State-Trait Anxiety Inventory (STAI) (IDATE), translated and validated in the Brazilian population by Biaggio et al. [17] as the Inventário de Ansiedade Traço-Estado (IDATE). The IDATE consists of two separate scales: trait anxiety and state anxiety, each containing 20 items with a response scale from 1 to 4 (1 = rarely, 2 = sometimes, 3 = frequently, and 4 = almost always). The total score for each scale was calculated by summing the scores of its items and ranged from 20 to 80 total points. The total points indicate the obtained anxiety levels: lower levels (20 to 40 points), medium levels (41 to 60 points), and high levels (61 to 80 points) [17].
Mood state
The athletes’ mood state and total mood disturbance (TMD) were measured using the Portuguese reduced and adapted version of the Profile of Mood States (POMS) questionnaire, validated by Viana et al. [18]. This reduced POMS consists of a 42-item scale with 6 subscales: Tension-Anxiety (T), Depression-Melancholy (D), Hostility-Anger (H), Fatigue-Inertia (F), Vigour-Activity (V), and Confusion-Disorientation (C). The response scale ranges from 0 to 4 (0 = never; 1 = a little; 2 = moderately; 3 = quite a bit; 4 = extremely). The following items have the same response scale, but inverted: ‘calm’ from subscale T, and ‘effective and competent’ from subscale C. To calculate the TMD, negative sub-scale scores are summed (T + D + H + F + C), the V subscale score is subtracted, and 100 points are added to the result [18].
Depression
The severity of depression symptoms in the athletes was measured using the Beck Depression Inventory II (BDI-II), which has been validated in the Brazilian population by Gomes-Oliveira et al. [19]. The BDI-II considers the athlete’s symptoms from the last 15 days. This tool consists of a 21-item scale with a response scale that ranges from 0 to 3, except for items 16 and 18. The total score of the scale can range from 0 to 63 and it can be interpreted with the following thresholds: minimal/no depression (0–13 points), mild depression (14–19 points), moderate (20–28 points), severe depression ( 29) [19].
Quality of life
Quality of life was measured using the Short Form-36 Health Survey (SF-36), translated and validated in the Brazilian population by Ciconelli et al. [20]. The SF-36 is a multidimensional tool composed of 36 items divided into 8 domains: physical functioning, role physical, bodily pain, general health perceptions, vitality, social functioning, role emotional, and mental health. Each domain has its score ranging from 0 to 100, with higher scores indicating better health status [20].
Procedures
The questionnaire was administered during a national-level Paralympic meeting organised by the Brazilian Paralympic Committee (BPC). The BPC previously approved the researcher’s presence at the event and direct contact with the athletes during the Paralympic Powerlifting competition. All questionnaires were administered through face-to-face interviews between the researcher and the athletes to ensure proper understanding and accurate completion of each instrument. All instruments were applied by the same licensed psychologist experienced in applying these instruments in multiple other studies.
The interviews were conducted approximately 60 min before the start of the competition, in a quiet room within the event facilities. Before questionnaire administration, all athletes provided written informed consent. During the interviews, the participants were encouraged to respond honestly based on their current emotional state. The purpose, procedures, and items of each questionnaire were thoroughly explained to ensure accurate understanding and interpretation.
Statistics
Data were presented using measures of central tendency, such as means ± standard deviations (SD) and 95% confidence intervals (95% CI). The Shapiro–Wilk test was performed to confirm the assumptions of normality. Student’s t-test was performed for independent measurements. To assess the effect size, a Cohen’s d value < 0.2 was considered a trivial effect, 0.2 to 0.6 a small effect, 0.6 to 1.2 a moderate effect, 1.2 to 2.0 a large effect, 2.0 to 4.0 a very large effect, and 4.0 an extremely large effect [21, 22]. Cohen’s d was calculated as the difference between the mean divided by the pooled SD to estimate the effect size for comparison between surveys [23]. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) software package, version 22.0 (IBM Corp, Armonk, NY, USA). The level of significance was set at p < 0.05.
Results
Figure 1 shows the results of the Beck Precompetitive Depression and Anxiety Inventory (CSAI-2).
Figure 1
Differences in depression (BDI-II) and pre-competitive anxiety subscales (CSAI-2) between female and male Para Powerlifting athletes: (A) Beck Depression Inventory (B) Cognitive Anxiety (C) Somatic Anxiety (D) Self-confidence
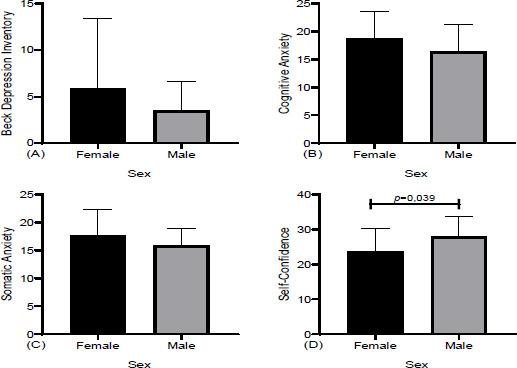
No significant differences were found in the Beck Depression Inventory. In Pre-Competitive Anxiety, a difference was found between the men (27.67 ± 5.81) and women (23.67 ± 6.55, p = 0.039, Cohen’s d = 0.711, moderate effect) only in Self-confidence (Figure 1D).
No difference was observed between the men and women in either trait or state anxiety.
Figure 3 shows the results between the genders in the different domains of the mood test (POMS).
Figure 2
Differences in trait and state anxiety (IDATE) between male and female Para Powerlifting athletes:
(A) Trait anxiety (B) State anxiety
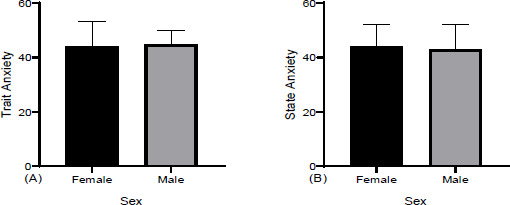
Figure 3
Differences in mood states (POMS) between male and female Para Powerlifting athletes: (A) Tension-Anxiety, (B) Depression-Discouragement, (C) Anger-Hostility, (D) Fatigue-Inertia, (E) Mental Confusion-Disorientation, (F) Vigour-Activity
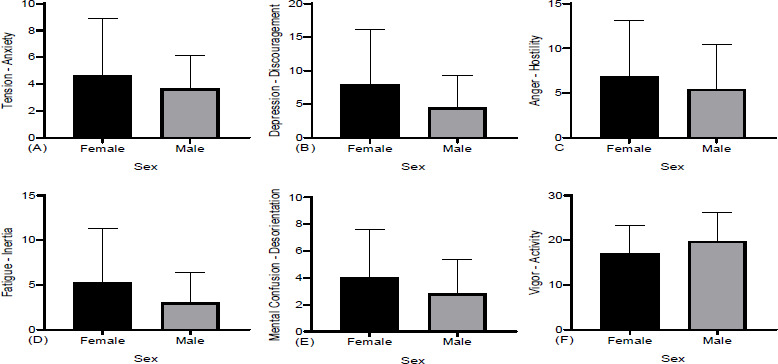
No differences were found in the various POMS domains, Tension-Anxiety, (B) Depression-Discouragement, (C) Anger-Hostility, (D) Fatigue-Inertia, (E) Mental Confusion-Disorientation, and (F) Vigour-Activity, between the males and females.
Figure 4 shows the results related to moods (POMS) and the total value of the mood scale.
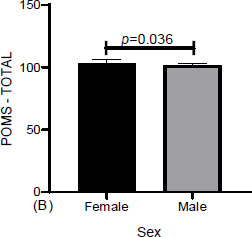
Differences in mood (POMS) were found between the men (101.69 ± 1.69) and women (103.27 ± 2.69, p = 0.036, Cohen’s d = 0.726, moderate effect).
Figure 5 presents the results of the SF-36 quality of life questionnaire and its domains.
Figure 5
Differences in quality-of-life domains (SF-36) between male and female Para Powerlifting athletes: (A) Functional Capacity, (B) Limitation of Physical Aspects, (C) Pain, (D) General Health Status, (E) Vitality, (F) Social Aspects, (G) Emotional Aspects, (H) Mental Health
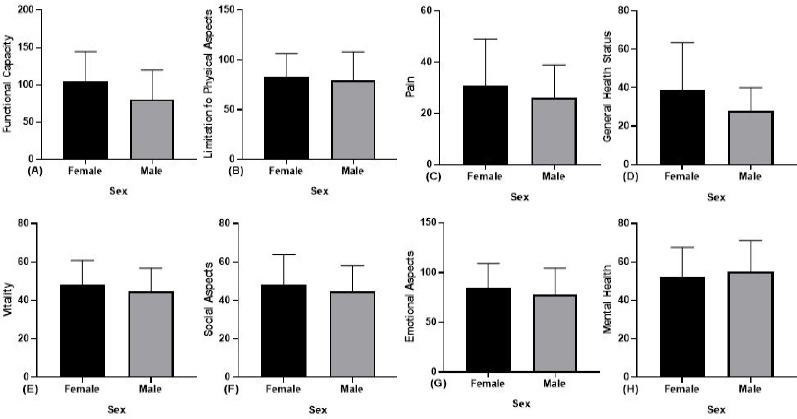
No significant differences were found in any quality-of-life domain measure resulting from SF-36 (Figure 5).
Discussion
Our study aimed to compare measures of mental health and quality of life between male and female Para Powerlifting athletes in a sports competition environment. Our main findings are that males reported higher self-confidence than female athletes after the competition; no differences were found between genders on anxiety measures; female athletes reported a higher total mood disturbance than males, but no differences were found in the six mood state dimensions; and no differences were found in depression and quality of life between the male and female Paralympic Powerlifting athletes.
The CSAI-2 results demonstrated that females present lower self-confidence than male athletes before the competition. This finding aligns with the results of Halilaj et al. [24], who found lower pre-competitive self-confidence in female than male able-bodied gymnasts. Similarly, O’Connor et al. [25] found lower self-confidence in female youth soccer athletes than their male counterparts in a high-performance environment. This phenomenon is replicated by athletes with disabilities, as is confirmed by a systematic review conducted by Pumpuang et al. that found that female athletes presented lower self-confidence than males [26]. These differences are thought to be due to psychosocial factors affecting female athletes, such as an inappropriate gender-role perception of the sporting task, sensitivity to social evaluation of their performance, and poor performance feedback [27]. Moreover, it appears that there is a relationship between self-confidence and experience in sports competitions, as experienced athletes tend to perceive the competition from a more positive perspective [28]. Although competitive experience was not assessed in our sample, it is possible that the women included in the study had less exposure to competitive environments and stimuli than their male counterparts, not only in sports contexts but throughout their lives. This is in line with the idea that males have a more competitive orientation to life than females [29].
Regarding anxiety measures, there is a general thought that female athletes with or without disabilities may experience higher anxiety than males [13, 26]. However, our study found no differences in pre-competitive somatic and cognitive anxiety measured by CSAI-2 or trait-state anxiety measured by IDATE. This contrary finding still aligns with those from other studies. Marín-González et al. [30] found no gender differences in somatic and cognitive anxiety among Olympic and Paralympic Colombian athletes, and Yaman et al. [31] also found no significant gender differences in trait-state anxiety among experienced able-bodied athletes from Istanbul. Conversely, some studies have presented results that differ from ours. Fernandes et al. [32] found that female able-bodied athletes presented higher cognitive anxiety than their male counterparts [32], and Kumari and Chauhan [33] found female able-bodied athletes present higher total anxiety levels than males. However, the sample of Fernandes et al. [32] was composed of amateur athletes, and the sample of Kumari and Chauhan [33] was composed of collegiate athletes. Considering that anxiety can be common in less experienced athletes, there is a possibility that the absence of differences in anxiety resulting from our study is related to the higher competitive level of our athletes [28].
Our study found no differences in the six mood state dimensions between males and females. However, the total mood disturbance (TMD) was higher in the female than in the male athletes. Contrary to our results, Abbas et al. [34] found that able-bodied women scored lower on depression and vigour than males, and female athletes reported higher TMD than males. TMD is a measure of emotional disturbance, psychological distress, or subjective well-being [35], suggesting that a higher TMD could indicate poor mental health. Our gender-specific difference found in TMD can be explained by the idea that female athletes are exposed to more gender-specific psychosocial stressors than males [36], in addition to female athletes reporting more mental health issues related to anxiety, depression, and distress than men [13]. In this vein, another confounding result from our research is that no differences were found in depression between the male and female athletes. Nonetheless, a similar result has been reported by Dita and Nopiyanto [37], who found no depression differences between male and female able-bodied colleague athletes. Therefore, it seems that negative mental health outcomes can vary in female athletes, and since there is a lack of literature about this subject in athletes with disabilities [14], we do not know if these variations are common in this population.
Our research also found no gender differences among athletes in any quality-of-life (QoL) domain. This result is contrary to Lee et al.’s [38] results, who found gender differences in QoL domains of elite Malaysian athletes with disabilities measured with the Short Form of the World Health Organization Quality of Life Questionnaire. In their case, males reported better social relationships and environmental health than female athletes [38]. Unfortunately, it seems that no more research has been conducted on this subject in athletes with disabilities. However, a study from Nowak et al. that included professional Polish able-bodied athletes also shows that males have a higher QoL score than females [39]. Nonetheless, in line with our findings, Narwal found no gender differences in the QoL of able-bodied Indian athletes [40]. A possible explanation for the lack of gender differences in QoL found in our study may be related to the adapted sport practice. A study by Zheng et al. [41] found that physical activity and sport practice enhanced the quality of life of athletes with disabilities, independent of their gender. Therefore, our findings may be related to an equalisation of QoL between genders in the Paralympic sport context.
Assessing the mental health and quality of life in athletes with disabilities is paramount, since differences between genders on these measures can be managed to achieve better competitive results for the whole team. The lack of research on mental health and quality of life in Paralympic athletes is an issue that hinders the understanding of the gender differences phenomenon in this population. To our knowledge, this is the first study comparing gender differences in Paralympic Powerlifting athletes and, together with the scarce research on psychological variables in this population, solid conclusions considering the particularities of Paralympic Powerlifting practice cannot be drawn. Finally, a limitation of our study is the lack of training and competitive experience in the athletes, as these variables could be related to the outcomes in self-confidence and anxiety.
Conclusions
Psychological factors are key for sport success and can vary between male and female Paralympic Power-lifting athletes, influenced by several factors. Our study shows that male Para Powerlifting athletes have higher self-confidence and lower mood disturbance than females, but both genders are equal in anxiety, depression, and quality of life measures. The scarcity of research on mental health and quality of life in athletes with disabilities hinders the complete understanding of these results. However, these gender differences can be caused by gender-specific psychosocial stressors and gender differences in exposure to competitive stimuli. In addition, involvement in a Paralympic sport context may be a cause of equal quality of life and mental health measures.