Introduction
Postural control is defined as reaching or returning to a state of equilibrium during standing in a quiet stance or in active situations and is achieved through the integration of sensory afferent inputs from proprioceptive, vestibular, and visual sources, which are processed in the upper centres of the nervous system [1]. If we consider the upright body biomechanically as a whole mass, the centre of mass (coM) in the human body corresponds to the midpoint of the pelvis (about Sacral 2) at the level of about 1 m above the ground [2]. balance is maintained by extending the gravity vector from the coM to the ground, positioned between the two feet and approximately 4–5 cm in front of the ankle axis, with the projection of the coM onto the support surface defined as the centre of pressure (coP) serving as a marker for postural stability [3]. The body is unstable in an upright standing position and tends to move constantly. In situations that destabilise the body, this is initially countered by a corrective rotational moment by the foot that is in contact with the support surface. The ankle helps the coM to stay in the base of support, and this requires adequate mobility of the ankle joint [4]. To maintain postural stability, ankle strategy is used frequently for low amplitude perturbations [5]. So, it can be said that there is a link between the ankle joint and postural control.
Effective postural control and balance are factors that contribute to the prevention of sports-specific injuries, particularly in the ankle joint. In volleyball, a sport characterised by rapid and frequent movements, it is very important to ensure postural stability. During volleyball-specific movements such as jumping and landing, blocking and spiking, lower extremity kinematics are important in absorbing the loads that can be placed on the musculoskeletal system and ensuring stability during the game [6]. Essential skills in volleyball, such as maintaining a balanced stance and effective postural control during ball contact, place great demands on ankle functions [7]. Under changing conditions, each athlete develops a different postural control mechanism against perturbations. Volleyball players generally use the ascending strategy to ensure their postural stability, where the support surface aligns the coM with the applied force, exerting an equal force in the opposite direction [8]. In other words, volleyball players maintain postural balance by adjusting from distal to proximal joints, particularly the ankle, in the loading model. This proves how important a central point the ankle is for volleyball players.
Ankle sprain, which are occurring more severely in women than in men, are particularly common in volleyball players [9–10]. Examining ankle sprains specifically, they are seen in volleyball players at a rate of 19%, while the general population sees a rate of 26 per 1000 people (0.216%) [11, 12]. The ankle joint serves as a dynamic link between the body and the ground, and the ability to adapt to different positions and movements during sports are related to postural control. The ankle joint plays a crucial role in maintaining postural control and preventing sports-related injuries, which is why it requires frequent evaluation, especially in female athletes.
More than one variable plays a role in the person reaching a state of equilibrium [13]. Joint mobility is important in order to provide the required range of motion (ROM) for the targeted movement to occur and to obtain appropriate joint mechanics. Joint stability is as important as joint mobility in order to avoid injuries. Since joint stability is dependent on sensory input from peripheral receptors, proprioception and other deep senses play a role in maintaining postural stability. Somatosensory inputs provide information about body position and movement and allow postural control to be achieved. Stability also ensures optimum muscle strength and proper co-contraction and coordination. Previous studies have shown that enhancing various functional parameters, such as strength, proprioception, and balance, can decrease the risk of injury and positively impact athletic performance [14, 15].
We started with the question of why the incidence of ankle sprains is higher in volleyball players, whom we know to have better muscle strength, than in healthy people. We reviewed the literature to investigate the variables of static stability and ankle functions that develop or change with volleyball-specific training, and the relationships between these variables in order to better understand the reason for this frequency of ankle injury in volleyball players, as compared to the population. However, ankle function assessments were not included in studies examining postural control in healthy volleyball players and their controls [1, 7].
To gain a better understanding of the specific abilities developed for the sport, it is important to investigate how volleyball experience affects ankle functions and postural control variables in athletes with stable ankles. We consider that volleyball players will have better results than healthy controls in terms of ankle function and postural control variables. We wonder what other factors are different in the ankle joint? To determine answers to these questions, we aimed to show how healthy controls and volleyball players differ in terms of ankle function, postural control, and deep senses (proprioception and vibration sense).
Another aim of our study was to determine the relationship between the evaluated ankle functions and postural control. because of the relationship between ankle injuries and impaired postural control, determining the variables that have the potential to affect postural control is beneficial for preventing ankle injuries.
Materials and methods
Study design
The study was performed as a single blind observational case-control study. The demographic and clinical information form was applied to the volunteers through a face-to-face interview. After completing the general information form, participants’ cumberland Ankle Instability Tool (cAIT) scores were assessed for study suitability. Selected individuals underwent a static balance assessment using a computerised stabilometer (ProKin-252) on a force platform. Postural control data were electronically recorded. Ankle evaluations included measuring active and passive ROM, joint position sense (JPS), vibration assessments, and strength measurements. All the clinical assessments were made by a single physiotherapist, who was blind to the allocation of groups to prevent bias. All participants were assessed individually. Volleyball players were evaluated on a day when they did not have training during the off season. The data were immediately recorded in an evaluation form. The entire evaluation, including rest, lasted approximately 45–60 min and the participants were not followed up afterwards. The eligibility criteria set for participation in the study are listed below.
Eligibility criteria
Inclusion criteria:
Female gender,
Aged between 18 and 25 years,
Having a score of 24 on cAIT,
Volunteering to participate in the study.
Additionally, for the volleyball group:
Having at least five years of volleyball experience [16].
Exclusion criteria:
Having neuromuscular diseases or vestibular or visual problems,
Having an orthopaedic injury located on the lower extremity,
Presence of acute or chronic pain,
Having suffered an ankle injury within the past year.
Additionally, for the control group:
Participating in individual or team sports, such as swimming, tennis, volleyball, soccer, etc.,
Participating in physical activity (all types of aerobic or strengthening training) for more than 150 min a week or more than 5 days a week (regardless of the duration) [5].
Participants
The sample size of the study was calculated using the G*Power program. Type 1 error value was set as α= 0.05 and power as (1- ) = 0.95. When the effect size (d value) was calculated from the reference article [16], the sample size for the independent sample t-test was calculated as 20 in each group and 40 in total. Twenty-five participants enrolled in the volleyball group (VG) from the Yeditepe University Volleyball Team, who trained three times a week for 60–90 min and participated in the University League (Unilig) and 24 students were enrolled in the control group (cG) from the Ye ditepe University Physiotherapy and Rehabilitation Department. After evaluating the eligibility of the people who volunteered to participate in the study; 5 of the volleyball players (1 having an ankle injury in the past year and 4 having a cAIT score 24) and 4 students (2 physically active and 2 having a cAIT score≤24) were excluded (Figure 1). After the number of people to be included in the study was sufficient, participant recruitment was stopped. The study was conducted at the Yeditepe University Physiotherapy and Rehabilitation Laboratory with a total of 40 participants (age: 21.18 ± 0.27, female) – 20 in each group.

Determination of ankle joint stability
The ankle joint stability was assessed using the cAIT, which evaluates the presence of pain and instability during various activities, such as walking, running, and jumping, on different surfaces [17]. cAIT distinguishes stable and unstable ankles from each other. The scale consists of nine questions about both right and left ankle joint functions and whether there is pain during the different activities mentioned above. A total of 30 points can be scored on this scale, with scores above 24 indicating increased stability and scores below 24 indicating increased instability. Participants with ankle stability scores 24 on the cAIT were included in the study and underwent additional evaluation procedures.
Assessment of postural control
Postural control was assessed using a computerised stabilometer (ProKin PK-252, Technobody, bergamo, Italy), which is proven to be a reliable tool and considered the gold standard method, in a bipedal silent, upright position with eyes open on a force platform [18]. before the test, participants were asked to try to stand still in silent, upright posture, and no warning was given during the test (Figure 2). The static stability test was performed for 30 s and was repeated three times. A rest period of 60 s was given between repetitions. The study measured the following variables: average postural sway velocity in the AP and ML directions (mm/s), sway area (mm2), and perimeter (mm) of the displacement of the centre of pressure (coP) [19]. The data were recorded immediately via computer and the mean value data were used for data analysis, where lower values indicated better postural stability.

Evaluation of ankle functions
All assessments of ankle functions were performed in the mentioned order on both extremities by the same physiotherapist after postural control assessment, with the extremity with which the participants preferred to kick a ball being considered the dominant side.
Range of motion
Dorsiflexion (DF), plantar flexion (PF), inversion (INVR) and eversion (EVR) ROM were measured with the help of a standard goniometer, both active and passively to evaluate the mobility of the ankle joint. For measuring DF and PF ROM, the participant laid supine on a bed with a thin pillow under the knee. The goniometer’s pivot point was positioned on the lateral malleolus, with its fixed arm parallel to the fibula’s lateral midline and its movable arm tracking the 5th metatarsal bone’s lateral midline. For measuring EVR and INVR ROM, the participant laid prone on a bed with the knee flexed at 90° and the ankle in a 90° neutral position. The goniometer’s pivot point was at the midpoint of the calcaneus, and the fixed arm, initially parallel to the midline of the sole, remained parallel to the ground throughout, while the movable arm followed the sole’s midline. All evaluations were repeated 3 times, and the average scores were recorded.
Joint position sense
Active JPS assessment was evaluated with the help of a standard goniometer at 105°, 120°, 130° and 140° DF, which were reference degrees. The assessment involved having the individual close their eyes while lying in a supine position, with a pillow supporting their legs and knees to promote knee flexion and calf muscle relaxation. The starting position of the foot was established at 145° of plantar flexion (PF). The ankle was randomly positioned passively at one of the reference degrees. The proximal arm was aligned parallel to the lateral midline of the fibula, the pivot point was placed on the lateral malleolus and the distal arm was set parallel to the 5th metatarsal, ensuring that the goniometer did not make contact with the skin during the evaluation. The person was expected to return the ankle to the reference degree starting from 145° PF and deviation from the reference degree was recorded [20]. There is a margin of error of up to ± 2° in ankle joint proprioception measurements [21]. This process was repeated three times, and the mean value was used for analysis.
Vibration disappearance threshold
The vibration disappearance threshold was assessed by placing a tuning fork (128 Hz) on the medial malleolus, 1st and 5th metatarsal heads. Upon hearing the vibrating sound immediately after striking the tuning fork against a solid surface, it was positioned at the designated reference point. With the help of a stopwatch, the seconds were measured until the person no longer felt the vibration sensation. Throughout the procedure, the patient’s eyes remained closed. Prior to the evaluation, a preliminary test was performed on the bone structure to help the patient become familiar with and develop their tactile sensitivity [22]. This process was repeated three times for each point, and the resulting average value was documented.
Isometric muscle strength
The maximum isometric strength as the highest force value (newton), at DF, PF, INVR and EVR movements of the ankle joint was evaluated by a manual dynamometer (JTech commander PowerTrack II; Jtech Medical, Salt Lake city, Utah, USA) [23]. Participants were shown the subtalar neutral position of the ankle and were asked to start each test from this position. Limbs that were not actively involved in the procedure were secured to the bed to eliminate any unintended movements. Prior to every measurement, the dynamometer underwent calibration. Evaluation positions were performed with maximal push or pull orientations with the dynamometer above the metatarsal heads according to previous research [24]. After the test was performed for 3 s in 3 repetitions with 10-second intervals and recorded, the highest force value (Newton) was used for statistical analysis.
Statistical analysis
The study analysis was carried out using the Statistical Package for Social Sciences (SPSS) 24 program. Descriptive statistics, such as mean and standard deviation (SD) were calculated. The Shapiro–Wilk test was used to analyse the normal distribution of the variables within the groups. Inferential statistics, including the Independent Samples T-test (for normally distributed variables) and the Mann–Whitney U test (for not normally distributed variables), were performed to examine differences between groups, whereas a Spear-man correlation Analysis was used to examine correlations between variables. correlation coefficients (r) were expressed as moderate for values between 0.4 and 0.6, and strong for values between 0.6 and 0.8. For all statistical analyses, a significance level of p < 0.05 was used [25].
Ethical approval
The research related to human use has complied with all the relevant national regulations and institutional policies, has followed the tenets of the Declaration of Helsinki, and has been approved by the Yeditepe University Ethics committee (approval No.: 202202159).
Results
Descriptive characteristics
All demographic variables were normally distributed within the groups (p > 0.05). When the demographic information of the participants was compared, there was no significant difference in the age and bMI, while the height and weight data were significantly different (Table 1).
comparison of ankle functions between groups
Table 2 illustrates the data and between-group differences for ankle functions. The active and passive ROM data for DF, INVR, and EVR, JPS at all reference degrees, vibration sensed through the 1st and 5th toe and DF and PF isometric muscle strength showed significant differences between groups for both extremities (p < 0.05). There was no significant difference in the other ankle function variables (active and passive PF ROM, vibration sensed through the medial malleolus, INVR and EVR isometric muscle strength) between the two groups (p > 0.05).
Table 2
Differences between groups in terms of ankle function variables
comparison of postural control between groups
In the results of the postural control variables, there were significant statistical differences between the two groups for all variables such as AP and ML sway velocity, perimeter and ellipse area variables (Table 3) (p < 0.05).
Table 3
Differences between groups in terms of postural control variables
correlation between ankle functions and postural control variables
The correlation between the ankle functions of the dominant (D) and non-dominant (ND) extremities and postural control variables are shown in Table 4.
Table 4
Correlation between ankle functions and postural control variables
[i] VG – volleyball group, CG – control group, D – dominant extremity, ND – non-dominant extremity, AP – anterior-posterior, ML – medial-lateral AROM – active range of motion, PROM – passive range of motion, JPS – joint position sense DF – dorsiflexion, PF – plantar flexion, INVR – inversion, EVR – eversion, MM – medial malleolus significant at p < 0.05
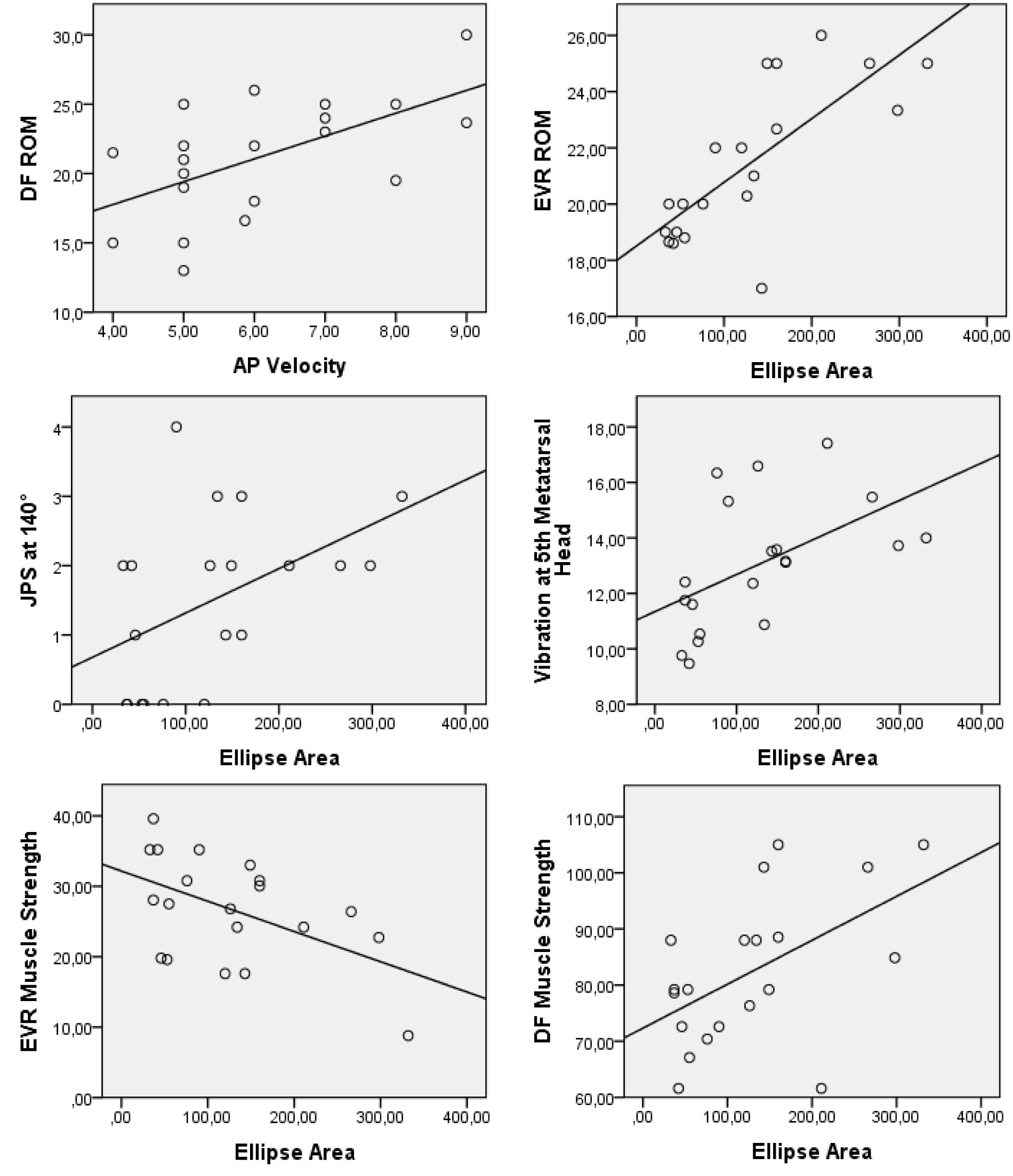
For the VG, AP sway velocity had significant correlations with the active DF, passive DF and passive EVR ROM. both ellipse area and perimeter variables had significant correlations with the active EVR ROM and there was a significant correlation between the ellipse area and passive INVR ROM as well. Also, significant correlations were observed between the ellipse area and the JPS at 130° and 140° and the vibration sensed through the 1st and 5th metatarsal heads. For the isometric muscle strength measurements, the ellipse area had a significant correlation with the DF and a negative correlation with the EVR directions and the ML sway velocity with the INVR direction at the VG (Figure 3).
For the cG, the AP sway velocity had a negative correlation with the passive EVR ROM. The ML sway velocity and perimeter variables had significant correlations with the passive PF ROM and the ML sway velocity was also significantly correlated with the passive INVR ROM. The cG had significant correlations between the AP sway velocity and the isometric strength in the INVR direction.
Discussion
The aim of this study was to evaluate different ankle functions and postural control variables in university-level volleyball players with stable ankles. To achieve this aim, we formed our sample group from female volleyball players as studies showing that females experience more severe ankle sprains than males, while also taking into consideration that physical fitness parameters of male and female athletes differ significantly. The results of the study have demonstrated that the volleyball players have better ankle ROM, JPS, DF and PF isometric muscle strength and postural control, whereas the controls had better vibration sensitivity. In addition, many ankle function variables were found to be related to the sway velocity and sway area.
In this study, we first compared volleyball players with the cG in terms of ankle functions. The ankle function ROM evaluation results (ankle DF, EVR and INVR ROM values) were found to be higher in the volleyball players, while no difference was observed between the volleyball players and the control group for the PF ROM. Regarding the ankle function JPS assessment, it was observed that volleyball players showed fewer errors in the reposition test than the controls. Regarding the vibration sense, which is considered to be another deep sense, there was a difference between the groups at the 1st and 5th metatarsal heads in favour of the controls, while the vibration sense taken from the medial malleolus region of the volleyball group was not different from the control group. In addition, the isometric muscle strength of the dorsiflexor and plan-tar flexor muscles of the volleyball players was found to be higher than in the control group, while the for INVR and EVR, the isometric muscle strengths did not differ between the groups.
When we look at the literature information on the ankle functions of volleyball players, many studies support our findings: DF, INVR and EVR ROM and DF and PF isometric strength are better in favour of volleyball players [16, 26–28]. It is generally accepted that the frequent training of specific movements in volleyball may lead to an improved ROM, JPS, and isometric strength, which was clearly seen in this study. but why was this improvement not observed in the PF ROM, the medial malleolus region vibration sense, and the INVR and EVR isometric strength values?
Volleyball players generally use the PF muscles with eccentric contraction, and so it is thought that a large ROM is not needed, in contrast to ballet dancers, who use frequent concentric PF contraction [26]. considering these results, the ROM could be changing according to the requirements of frequently repeated movements specific to volleyball with regular training. One study found that volleyball training improved the JPS in the knee joint compared to healthy controls [16]. According to the evaluation results of the vibration sense, which is accepted as another deep sense, there was a difference between the groups at the 1st and 5th metatarsal head, which was in favour of the controls in our study. We did not expect this result. No comparison has been made in the existing literature between the vibration sensitivity of healthy athletes and sedentary controls. The absence of a similar study in the literature makes it difficult to discuss this situation. However, we think that it could be explained by physical properties. Factors such as age and height can affect sensitivity vibration thresholds. Additionally, one early study found the vibration thresholds at the foot increases at a certain rate with every 10 cm increase in height [29]. Our study’s volleyball players had a higher mean height compared to the controls, which may explain our results. However, this does not explain the vibration sense result obtained for the medial malleolus region. Other studies on the sense of vibration are needed to explain it.
In the current study, it was shown that all postural control variables of the volleyball players were better than the cG. There are studies comparing the postural stability of both male and female volleyball players with healthy controls, and most of them reached the same conclusion as us [1, 7]. Athletes use different strategies than controls by making slight muscle adjustments to ensure a stable adaptation to the rapidly changing game. considering the need for postural stability required by the sport, the superior postural control ability seen in athletes can be easily explained.
In this study, we also examined the relationships between postural control and ankle functions. As postural control is identified as a risk factor for ankle injuries, investigating factors related to it is crucial in preventing potential injuries, particularly among athletes. Our study explored associations between postural control variables and various ankle functions in volleyball players. All the postural control variables of the volleyball players were found to be significantly better than the controls and also associated with some functions of the ankle. Especially in volleyball players, a relationship has been shown between ankle functions and AP sway velocity and ellipse area measurements.
Based on the results of our study, it was determined that there was a correlation between the active and passive DF ROM and the AP velocity variable, and between the active EVR ROM and the ellipse area for VG. Also, the passive PF ROMs of the controls were found to have significant correlations with the ML sway velocity and perimeter variables, which demonstrates that an increased ROM is correlated with poor postural control. If an increased ROM is associated with poor postural control, it can be safely assumed that an increased ROM may be a risk factor for ankle injuries. Previously, an increased EVR ROM has been identified as a potential risk factor for injuries [30]. In contrast, a reduced active DF ROM has been shown to be a predictor of ankle injuries in volleyball players. This is because an insufficient DF ROM in the ankle joint can result in a rigid landing following a jump, thereby elevating the likelihood of ankle sprains [31, 32]. It is challenging to draw definitive conclusions regarding average joint mobility or flexibility values. Since both looseness and stiffness of the joint cause stability problems, these results could be showing that an optimal ankle ROM is needed to ensure postural stability and eliminate the risk of ankle injuries. In addition to all these, this study sought to answer the question of what the optimal DF and PF ROM is in volleyball players.
There was a significant correlation between the JPS at 130º and 140º with the ellipse area for the non-dominant extremity of the volleyball players, which indicates that the increase of error at the JPS assessment is correlated with the increase of the ellipse area of the displacement of coP. One study that agrees with our results showed that ankle proprioception was a determiner of static stability [33]. Research shows that better JPS results may decrease the risk of a possible ankle injury [34]. Therefore, it should be taken into consideration that athletes with better proprioceptive abilities will have a lower risk of injury, and assessing postural control could be a marker for this.
According to our study, the vibration threshold and ellipse area were found to be correlated at the 1st and 5th metatarsal heads for volleyball players. In other words, this shows that as the ellipse area increases, the postural control ability decreases and the vibration threshold increases. Studies investigating the relationship between vibration sensitivity and postural control were generally conducted with the elderly and pathological groups and found a negative relationship between variables, as our study [35]. Height, weight and age are some of the factors that have been proven in previous research to have an effect on vibration sensitivity [36]. In addition to the scarcity of studies on this subject, it is very difficult to comment because the samples of existing studies and the sample we included in our study have very different demographic and anthropometric characteristics.
Muscle strength and effective co-contraction of the antagonist muscles provide the necessary coordination and thus ensure efficient joint stability to reduce the risk of possible injuries [37]. We found that there was a significant correlation between the dorsiflexor isometric muscle strength and the ellipse area of the volleyball players, and between the invertor isometric muscle strength and the AP and ML sway velocity of both the volleyball players and controls. Our study contrasts with previous research, which found that the isometric muscle strength of the dorsiflexors and plan-tar flexors positively impacts the postural control in healthy young individuals [29]. However, a study on 655 athletes from 9 sports found a positive correlation between these muscles’ strength and the sway velocity during a single-leg stance [38]. Higher muscle strength may impede postural control in athletes, but for those with average or lower strength, values approaching the mean may improve control. Optimal dorsiflexor and plantar flexor strength, in particular, can positively impact postural control by controlling AP sway during stance and thus can be beneficial in reducing the risk of injury. The evertor muscles contribute significantly to ankle stability. A significant negative correlation between the evertor isometric muscle strength and the ellipse area was found for volleyball players. In accordance with our study, a negative correlation was found between the evertor muscle strength and the AP displacement of the coP of 19 recreational athletes who have a history of ankle sprain [39]. It is possible that volleyball players may develop a postural control mechanism based on the strength of the evertor muscles.
The limitations of the present study are that only participants with stable ankles were included in the study. In order to understand the relationship between ankle functions and postural control in depth in the presence of pathology, a group with ankle instability can be added to future studies. Although the lack of objective evaluations of the ankle functions used in the study may have affected the outcomes, it was an advantage that they were convenient and easily accessible methods for use in the clinical settings. Also, the diversity of the postural control variables, individual differences and the scarcity of similar studies in the literature made it difficult to reach clear conclusions. However, in the light of the very few studies carried out with different populations in the literature and reaching contradictory results, it is assumed that with regular volleyball training, ankle functions can adapt to the needs of the sport of volleyball. It should be assessed regularly when taking the relationship between ankle functions and postural control into consideration, to prevent possible sport-specific injuries.
Conclusions
Our results have demonstrated that the volleyball players had better ankle ROM, JPS, DF and PF isometric muscle strength and postural control, whereas the controls had better vibration sensitivity. What is clearly demonstrated in this study in terms of the ankle functions of volleyball players is that the ankle PF ROM values, vibration sensation in the medial malleolus region, as well as the ankle INV and EVR isometric muscle strength are no different from the control group. This result may explain why volleyball players are vulnerable to ankle sprains, considering that their load on the ankle area is much higher. In addition, many ankle function variables were found to be related to the sway velocity and sway area of displacement of the coP. Since effective postural control reduces the risk of injury, evaluating the ankle functions that affect postural control will be beneficial in contributing to preventive rehabilitation. We believe that more detailed studies should be performed, especially to understand the postural control abilities of volleyball players.