Introduction
The prescription of exercise training intensity is an important goal within the sports and fitness community. Exercise intensity is commonly categorized into three domains: moderate, heavy and severe intensity [1]. These domains are categorized by oxygen uptake (VO2) kinetics and and blood lactate (HLa) responses. During moderate exercise, a plateau in VO2 occurs, which is below (<) the first ventilatory threshold (VT1), while HLa concentrations remain below the lactate threshold (LT). During heavy exercise, a ‘slow component’ of VO2 is observed, characterised by a delayed steady-state, and a rise in HLa above baseline, followed by a subsequent plateau. In this domain, both VO2 and HLa exceed (>) the VT1 and LT. During severe exercise, the ‘slow component’ of VO2 is present without a steady-state, and HLa continues to rise. In this domain, VO2 is above the second ventilatory threshold (VT2), and HLa rises inexorably towards the point of fatigue [1, 2].
The response to training varies across intensity domains, with each contributing distinct fitness benefits. The moderate-intensity domain is associated with aerobic adaptations, such as increased mitochondrial density and capillarisation, which enhance the VO2. This domain provides gains in cardiorespiratory fitness, making it suitable for sedentary individuals and for building an aerobic base in athletes [3]. In contrast, the heavy and severe intensity domains allow exercisers to achieve improvements in maximum VO2 (VO2max) and neuromuscular function, which support higher levels of performance. However, these domains also involve greater physiological stress and require more recovery [3]. Most individuals experience negatively accelerated (diminishing returns) gains in fitness with increased training volume and/or intensity [4-7]. Contemporary practice often focuses on keeping training intensity low (moderate-intensity domain) for the first few weeks [4, 7, 8]. Recent evidence, based on the magnitude of homeostatic disturbance driven signalling [9], suggests that training in the heavy or severe intensity domains results in larger increases in VO2max and threshold [5, 6, 10, 11] in non-athletic individuals. However, even in well-trained or athletic populations, where the motivation to achieve maximal gains is high, approximately 70-80% of training is typically performed in the moderate-intensity domain [2, 12-17]. In these groups, about 20-40% of training sessions are recommended to occur in the heavy [2, 12-17] or severe intensity domains.
While direct measurements of heart rate (HR), HLa or VO2 are precise tools for monitoring intensity, they are often impractical for non-elite athletes. Therefore, in recent years, researchers have promoted the development of simpler methods, such as the rating of perceived exertion (RPE) [8, 18-21] and the Talk Test (TT) [22-37]. The TT is based on the relative ease with which a person can speak while exercising. Originally described as a tool for mountaineers, it was based on the simple rule to “climb no faster than you can talk” [32]. The TT is thought to work because the reduction in breathing frequency associated with speech, which occurs at a time when breathing frequency would normally increase with higher intensity (e.g., >VT1, VT2), leads to a reduction in carbon dioxide production (VCO2), an increase in the arterial partial pressure of carbon dioxide (PaCO2) and thus reduced comfort during speech [38]. Despite using a variety of exercise protocols and verbal anchors, the TT has proven useful as a guide to training intensity in populations ranging from patients [35-37] to healthy sedentary individuals [8, 23, 29], as well as athletes [20, 25, 26, 33]. During the TT, the subject is asked to recite a standard paragraph out loud. They are then asked, “Can you speak comfortably?” There are three possible responses to this question: “Yes”, “Not sure” and “No” [23-25, 30]. Experience shows that the response is usually clear and definitive. When individuals can speak comfortably during exercise, the intensity is typically below VT. The last exercise stage at which participants can still speak comfortably is referred to as the last, while the stage immediately preceding this, where they can just begin to speak comfortably, is called the last positive-1 (LP-1) [23-25, 30]. Typically, the LP-1 stage corresponds to approximately 75% HRmax, an RPE of ~3 and a TT score of ~1/3. The LP stage corresponds to ~80% HRmax, an RPE of ~4 and an average TT score > 0.90 in a variety of studies. During the EQ stage, individuals are typically exercising at an intensity close to the VO2 at VT during incremental exercise. In fact, the EQ stage corresponds to ~85% HRmax, an RPE of ~5 and an average TT score of ~2.5/3. If individuals are clearly uncomfortable when trying to speak (answering “No”), they are typically at or above VT2. This stage is defined as the negative (NEG) stage [23-25, 30].
Exercise prescriptions based on different TT stages [8, 18-21], as well as HR [4, 7, 12-17, 39, 40], HLa [14-17, 25, 27, 33, 40] and RPE [8, 18-21], are established based on responses observed during incremental exercise. However, translating these results to steady-state training presents challenges [23, 30, 39, 40] due to physiological “drift”, particularly during >VT1 exercise, where the VO2 slow component predisposes the body to cardiovascular or metabolic drift [41-43]. While studies have validated the use of the TT in diverse populations [22, 25, 30, 31, 37], most focus on its utility during incremental testing rather than its application to prolonged (60 min) steady-state exercise. This limitation is critical because physiological responses observed during incremental tests may not directly translate to steady-state training conditions, particularly during >VT1 exercise. Studies from our laboratory, in patients with heart disease [22, 35], healthy sedentary individuals [23] and recreational and high-level athletes [25, 27, 33], have shown a predictable drift using the TT. Among the TT stages, LP-1 and LP correspond to conditions consistent with the moderate-intensity domain [33], showing minimal drift during steady-state exercise (from 20-40 min duration) and stable RPE [29]. Therefore, while the simplicity of prescribing steady-state training using the TT seems appealing, it is essential to evaluate the magnitude of physiological drift during prolonged steady-state exercise to translate the responses observed during incremental testing to protracted steady-state training. Accordingly, the purpose of this study was to evaluate the ability of the workloads at the LP-1, LP and EQ stages of the TT, observed during incremental exercise, to predict exercise responses during 60 min of steady-state exercise training in well-trained non-athletes.
Material and methods
Study design
This study was an observational, randomised crossover study designed to evaluate physiological responses during prolonged steady-state exercise at different intensities, based solely on TT responses during incremental exercise. Each participant completed three 60-min steady-state exercise bouts (LP-1, LP and EQ intensities) in a randomised order, with adequate rest (4872 h) between sessions to minimise carryover effects. The study was conducted in a controlled laboratory environment at the university.
Subjects
The subjects were well-trained, young adult, nonathletes (6 male, 6 female; Table 1), recruited from a university hiking club. They exercised 3-4 days per week, primarily hiking in the forest for 1-3 h per session. Except for very low-intensity “turkey trot” type events, the participants did not regularly compete, which is why they were classified as “non-athletes”. Additionally, they kept extensive records of their training, including frequency, with a non-specific comment regarding the intensity of their hiking, describing it as “somewhat hard” (14 or 4 on the classic or category ratio version of Borg’s RPE scale). The local hiking trails were undulating, with occasional higher-intensity efforts, although the overall training volume (> 7 h per week) at a “somewhat hard” intensity supports the description of this group as “well-trained”. The subjects were healthy students with no medical contraindications or medical treatments that might interfere with normal physiological responses to exercise. This sample is similar to the group studied by Jeans et al. [33], although they typically performed longer training sessions and did not usually participate in competitions.
Experimental procedures
The experiments were conducted at the same time of day (13:00-18:00) in an environmentally controlled room, maintained at 19-21°C with a relative humidity of ~20-40%. A low-intensity airflow was directed over the subjects for comfort. Subjects were provided with water or sports drinks ad libitum according to their personal preferences. None of the participants were smokers, and all arrived at the laboratory after fasting for at least 3 h. The first measurement was taken at 10 min, immediately following an 8-min ramped warm-up. Subsequent measurements were taken every 10 min, without interrupting the exercise.
Participants performed two incremental exercise tests (2-min stages) to measure VO2 and three 60-min bouts of steady-state exercise by walking uphill. During incremental exercise, they performed one test with measurement of respiratory metabolism through open-circuit spirometry (AEI Inc, Pittsburgh, PA), following a modified Balke-type protocol (speed = 1.6 or 1.8 m • s-1, based on individual preference) with a +2% elevation increase every 2 min. This protocol was designed to better match the individuals’ regular walking conditions, as they primarily train by hiking in the forest on hilly terrain. On a separate day, using the same exercise protocol, they performed the TT at rest and during the last 30 s of each stage, rating their speech difficulty. The TT involved reading a 31-word passage that was culturally familiar in the USA: the “Pledge of Allegiance”. This passage is commonly learned by individuals by the age of 8. To ensure accessibility, a cue card with the text was available, but it was never needed during the study. Additionally, many participants had previously been involved in similar studies in our laboratory, making the procedure familiar to them.
Speech difficulty was assessed by asking participants, “Can you still speak comfortably?”. Workloads representing the LP-1, LP and EQ stages (nominally equivalent to VT1 [30]) were noted. These intensities were then repeated during randomly ordered 60-min exercise bouts (8 min of an incremental warm-up + 52 min in steady-state at the speed/grade associated with the desired TT response). The steady-state bouts were separated by 48-72 h. Although subsequent studies have shown that the 31-word TT variant tends to prescribe training intensities at the EQ intensity that may be too difficult to sustain [28], this version remains widely used due to its simplicity. We [30] have generally used 2-min stages because shorter stages were adversely affected by the more frequent repetition of the TT.
All subjects completed all exercise bouts. HR (Polar Electro, Lake Success, NY), HLa (Lactate Pro, Nova Biomedical) and RPE (category ratio Borg scale) were measured at 10, 20, 30, 40, 50 and 60 min. The TT score (1 = still speaking comfortably, 2 = speech is somewhat difficult, 3 = speech is not comfortable) was obtained at the same intervals. We did not directly measure respiratory gas exchange during the steady-state bouts, as we did not want the breathing apparatus to interfere with perceptions of speech comfort. In fact, because we used a scuba-type mouthpiece rather than a facemask, intelligible speech was nearly impossible. Previous studies during both incremental and steady-state exercise have shown similar physiological responses with and without the measurement of respiratory metabolism [38]. This finding supports our assumption that measurements obtained with a mouthpiece are comparable to those without it.
Statistical analyses
Comparisons of responses in the outcome measures were made using repeated measures ANOVA to test the hypothesis that the stability of the drift in responses during the exercise training bout would depend on TT responses during incremental exercise. The Tukey test was applied to post-hoc evaluations when justified by ANOVA. Statistical significance was set at p < 0.05.
Results
The physiological responses regarding % HRmax during the 60-min steady-state exercise bouts at inten sities corresponding to LP-1, LP and EQ from the incremental exercise test are presented in Figure 1.
Figure 1
Percentage of maximum heart rate (% HRmax) response during the 60-min steady-state exercise bouts at the intensities associated with the last positive-1 (LP-1), last positive (LP) and equivocal (EQ) exercise intensities during incremental exercise
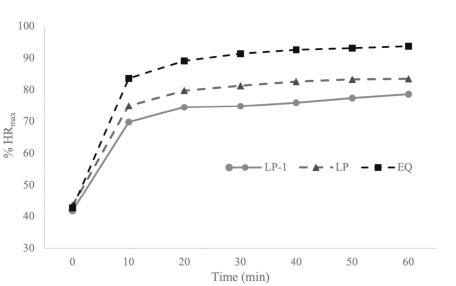
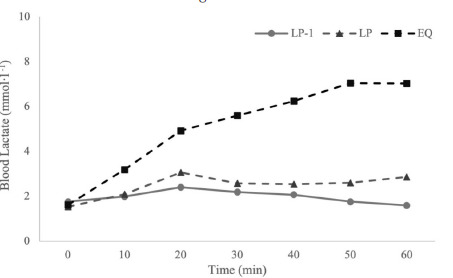
There was relative stability in the outcome measures during both LP-1 and LP intensity steady-state bouts, although the magnitude of drift was significantly greater during the LP bout compared to the LP-1 bout. HR was significantly higher, by 5-10% HRmax per TT intensity category. This led to a near-maximal final HR after 60 min at the EQ intensity. HLa exceeded the criteria for the maximal lactate steady-state (MLSS) [27] during the EQ intensity bout, with HLa reaching an absolute value of ~7 mmol • l-1. HLa remained below 3 mmol • l-1 and was not significantly different between the LP-1 and LP steady-state bouts (Figure 2).
Figure 2
Blood lactate (HLa) response during the 60-min steady-state exercise bouts at the intensities associated with the LP-1, LP and EQ exercise intensities during incremental exercise
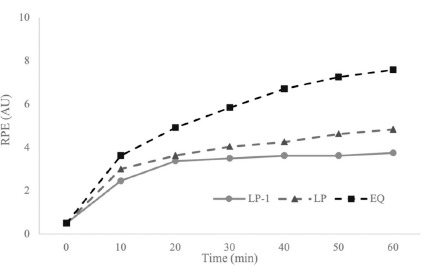
RPE drifted upward during the steady-state bouts, with the magnitude of drift significantly greater during the EQ intensity bout. This replicates previous findings using RPE [29]. As shown in Figure 3, during the LP-1 intensity steady-state bout, RPE remained below 4 and increased only slightly, without significant differences during the LP bout.
Figure 3
Rating of perceived exertion (RPE) response during the 60-min steady-state exercise bouts at the intensities associated with the LP-1, LP and EQ exercise intensities during incremental exercise
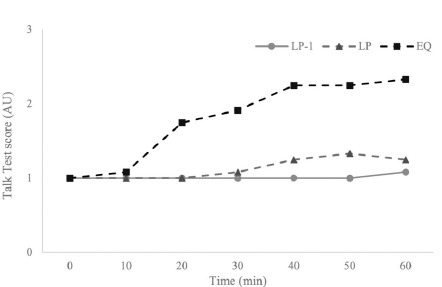
The TT score also drifted significantly upward in both the LP and EQ bouts, although it remained near comfortable speech levels for most participants during the LP-1 bout. the TT score was significantly higher during the EQ steady-state bout, as shown in Figure 4.
Figure 4
Talk Test (TT) score responses during the 60-min steady-state exercise bouts at the intensities associated with the LP-1, LP and EQ exercise intensities during incremental exercise
Means and standard deviations for % HRmax, RPE, HLa and TT score during the 60-min steady-state exercise bouts at the intensities corresponding to LP-1, LP and EQ are presented in Tables 2, 3 and 4, respectively.
Table 2
Means and standard deviations of the physiological responses during the 60-min steady-state exercise bouts at the intensities associated with the LP-1 exercise intensity
Table 3
Means and standard deviations of the physiological responses during the 60-min steady-state exercise bouts at the intensities associated with the LP exercise intensity
Table 4
Means and standard deviations of the physiological responses during the 60-min steady-state exercise bouts at the intensities associated with the EQ exercise intensity
Discussion
The main finding of this study was that during prolonged exercise, with absolute intensity defined based on TT responses during incremental exercise, the LP-1 intensity and, to some degree, the LP intensity, resulted in stable responses over 60 min of exercise. this corresponds to a physiological status consistent with the moderate-intensity exercise domain. These results are similar to those observed in recreational runners during a 40-min bout [33] and are substantially similar to those seen in less well-trained patients [35] and healthy sedentary individuals [23] during 20-min exercise bouts. For instance, Foster et al. [23] reported minimal physiological drift in HR, HLa and RPE during exercise bouts at these intensities, even in sedentary individuals, supporting their use in populations with low fitness levels. In physically active populations, such as the recreational runners studied by Jeans et al. , the LP and LP-1 intensities have also been shown to facilitate moderate-intensity exercise with minimal drift during 40-min bouts. Our study extends these findings by showing that stable responses persist during 60-min bouts, suggesting that the LP-1 intensity is applicable even for prolonged exercise in both sedentary and well-trained individuals. this is important because exercise in the moderate-intensity domain can be sustained for prolonged periods and may be required either to complete early exercise bouts in less active individuals/patients or to tolerate longer training efforts in more athletic individuals [17, 27, 29]. Indeed, while more well-trained individuals can apparently tolerate the LP training intensity [33], the current and previous results suggest that the LP-1 intensity has broader applicability. While this same information can certainly be accessed by direct measurements of HR or HLa, it is much easier to obtain using simple markers such as the TT and/or RPE.
Training in the moderate-intensity domain is generally below competitive intensity for most endurance sports (e.g., running, cycling, speed skating, swimming, rowing). Prolonged training in this domain is likely to enhance mitochondrial density and capillary network formation, sufficient to support oxidative energy supply in type I fibres. This can function not only as an immediate source of ATP but also to clear metabolites from adjacent type II fibres.
The TT can also potentially be used to define other training zones. The current data, as well as data from well-trained runners [33], suggest that the heavy training intensity domain, >VT1 <MLSS, can be estimated from the intensity at the EQ stage of the TT, particularly during steady-state exercise. Potentially, the severe training intensity domain could be estimated from the NEG stage of the TT [27], although the EQ stage of the TT specifically corresponds to VT1 during incremental exercise [30]. This suggests that a very simple approach to evaluation can be used to define the broad structure of training intensity distribution with reasonable accuracy.
This approach is supported by earlier findings from Woltmann et al. [27], who showed that, in sub-elite runners, the pace at the NEG stage of the TT could be tolerated for about 30 min, yielding near-maximal HR, RPE ~9 and HLa ~9 mmol • l-1, which approximates a 10 km race pace for athletes [44]. We speculate that the TT pace at NEG+1 would correspond to the velocity at VO2max, which awaits experimental confirmation. Thus, with minimal extrapolation, it seems feasible to identify intensities around which to base an entire training programme, solely based on TT responses during submaximal exercise.
An additional advantage of the current approach is that steady-state training intensities can be defined largely through submaximal exercise testing. This approach is less aversive than maximal testing, likely more time-efficient and can essentially be done as a warm-up for any training session. We have previously suggested that responses during submaximal exercise, conducted as part of the warm-up, could provide an index of fitness and readiness to train throughout the training year [45]. Furthermore, although the risk of exercise testing, even in patients, is low [22, 46], the fact that the current evaluative system stops at the EQ stage of the TT (which corresponds to the momentary intensity of VT) means that the risk of adverse responses, even in individuals likely to develop ischaemic responses during incremental exercise, is low [22, 46].
Our protocol used 2-min stages to define TT responses during incremental exercise. Previous studies [8, 30] have shown that the VO2 at the EQ stage of the TT approximates VT1. However, the steady-state VO2 requirement of a particular workload is unlikely to be reached in less than 3 min [41-43]. Accordingly, it is not surprising that the EQ stage showed evidence of considerable drift in cardiovascular/metabolic responses, as the steady-state requirement of this stage was likely above VT1, and into the heavy exercise domain, which typically has an observable slow component of VO2 [41]. The drift observed at the EQ stage of the TT is a physiological phenomenon expected when exercise intensity exceeds VT1. As exercise intensity increases beyond VT1, there is a transition from predominantly aerobic metabolism to a mix of aerobic and anaerobic energy systems, leading to a drift in VO2, HR and HLa levels [3]. The slow component of VO2, which becomes more evident at higher intensities, is a key factor contributing to this drift. this drift at the EQ stage indicates that maintaining a steady-state becomes difficult as exercise intensity exceeds VT1, particularly during longer-duration bouts. the drift in cardiovascular and metabolic responses at this stage suggests that exercise at the EQ intensity, especially during prolonged sessions lasting up to 60 min, may not be sustainable without fatigue and metabolic strain.
The TT procedure presented here appears to have considerable universal value at the intensity associated with LP-1. It remains to be seen whether it could further translate to prescribing exercise intensities for elite athletes or for exercise bouts lasting longer than 60 min. Certainly, the advice of Seiler [17] regarding the concept of polarised training, emphasises that athletes need to exercise at a pace slow enough to accumulate sufficient duration for building endurance. In this regard, the LP-1 stage of the incremental TT is likely to be more applicable than the LP stage.
Future research
While the current study provides valuable insights into the use of the TT for prescribing exercise intensity, particularly the LP-1 intensity, further research is needed to explore its applicability in other populations and for different volumes of exercise. Specifically, the effectiveness of the LP-1 intensity in elite athletes and during long-duration events (i.e., >60 min) remains to be fully determined. In elite athletes, who typically have higher VO2max, the physiological responses to exercise may differ, as these individuals tend to tolerate higher intensities and exhibit different VT thresholds, potentially allowing them to reach higher TT stages. Moreover, future studies could investigate the use of the TT in high-volume exercise. For instance, the utility of the LP-1 intensity in events lasting longer than 60 min, such as marathons or ultramarathons, could help clarify whether it remains a reliable tool for maintaining steady-state exercise without excessive fatigue or drift.
Conclusions
The TT is a simple tool for prescribing exercise intensity. It is effective not only during incremental exercise for identifying the VO2 at VT1 [8, 30] but also for defining training intensity domains during steady-state exercise. The present study suggests that a simple submaximal evaluation, based on TT responses during incremental exercise, can define the workload necessary to provoke appropriate training intensities. The findings indicate that the intensity associated with the LP-1 stage of the TT may be suitable for steady-state exercise at an intensity below VT1. The LP-1 intensity consistently and reliably predicts an exercise intensity within the moderate-intensity domain during steady-state exercise across multiple groups of exercisers. These findings suggest consistency of response to exercise ranging from patients and fitness participants to recreational athletes and even elite athletes. Using the TT to monitor responses at the LP-1 intensity can help maintain a training load without overloading the cardiovascular system, which is particularly important for individuals with chronic conditions or sedentary populations. Moreover, the TT can be applied to prescribe exercise intensity for endurance training, helping athletes or fitness enthusiasts optimise their training loads by ensuring they perform within the moderate-intensity domain without risking overtraining. Further, the results align with the advice given to mountaineers, originally attributed to John Grayson in the 1930s [32], which advocates, “climb no faster than you can talk”.