Introduction
Football requires both linear movements and movements involving preplanned or reactive changes in direction, depending on game situations. Agility, defined as “a rapid whole-body movement with a change of speed or direction in response to a stimulus” [1], plays a central role in these movements and is critical in both offensive and defensive manoeuvres. As such, agility can be viewed as a composite skill, incorporating components like change of direction speed (CODS) and perceptual-cognitive abilities [2]. CODS refers to a rapid, intentional, and preplanned change in direction or velocity, distinguishing it from agility that involves responding to external cues [3]. CODS and agility are distinct skills [4], however, CODS is preplanned, and agility involves reacting to a stimulus.
In football, CODS is instrumental for players to accelerate, change body direction, and rapidly decelerate to increase the chance of players winning one-onone duels or performing effective defending manoeuvres during the match [1]. Cultivating these skills is especially crucial for youth soccer players, as it can significantly impact their long-term performance and career development [5]. Nonetheless, the nuances between agility and CODS are often overlooked in sports research, many studies in the sports literature claiming to investigate agility are actually examining CODS, focusing on preplanned movements rather than agility [6].
Enhancing CODS can be targeted through various training methods, one of which is small-sided games (SSGs). SSGs present a distinct football approach, resembling the 11 versus 11 format but involving fewer players on a field adapted to the player count or specific training goals. Regarded favourably, SSGs are recognised for enhancing a player’s physical [7], technical [8], and tactical skills [9]. Moreover, they are recommended for refining decision-making and player autonomy by offering diverse scenarios that demand prompt and effective choices [10], ultimately contributing to increased enjoyment during training sessions [11].
Despite their popularity, there needs to be more research on how SSGs compare with other training methods in improving CODS in youth soccer players. A previous review found no significant differences between SSGs and running-based high-intensity interval training (HIIT), though the HIIT group showed greater within-group improvements [12]. HIIT involves alternating short bursts of intense activity with rest periods or lower-intensity exercise. However, SSGs have only been compared with HIIT, leaving a significant gap in understanding how it compares to other training methods such as plyometrics, strength training, or technical drills on CODS performance. Another SRMA on team sports, which included a very limited number of soccer studies, revealed that SSGs, compared with control groups (CoN), had a larger beneficial effect on CODS performance [13].
Given the widespread popularity and effectiveness of SSGs, and the gaps in existing research, this systematic literature review and meta-analysis aims to explore the influence of SSG intervention programs compared to various other training methods on CODS performance among young soccer players. To address this question, the following objectives have been established: (i) to identify and synthesise studies focused on enhancing CODS through SSGs, (ii) to evaluate the efficacy of SSG interventions compared with other training methods on CODS, and (iii) to pinpoint existing gaps in the literature concerning the targeted subjects.
Material and methods
The systematic review strategy was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines [14]. The protocol was published in the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) with the identification number INPLASY202440006.
Eligibility criteria
The inclusion criteria for this systematic review were as follows: (i) healthy male or female soccer players under the age of 19 (prior to reaching full maturation) [15], (ii) SSG programs lasting a minimum of 4 weeks, inclusion of SSGs combined with other programs was acceptable, (iii) presence of a passive or active control group, (iv) availability of pre-post intervention values for CODS, and (v) peer-reviewed original full-text articles written in English.
Search strategy
Electronic databases, such as Web of Science (01.03. 2024), PubMed (02.03.2024), and Scopus (04.04.2024), were systematically searched for relevant literature without applying an age range filter or other options to filter the results. The search strategy included the following keywords: (soccer oR football) AND (youth oR young oR child oR adolescent oR junior) AND (agility oR change of direction oR directional changes) AND (small-sided games).
Study selection
We imported titles and abstracts retrieved by the searches into Rayyan (a web and mobile app for systematic reviews), which automatically detected duplicates which were manually deleted by the authors. The screening process for study inclusion was conducted independently by two authors: I.N. and V.P. In cases of discrepancies, the third author, IM, was consulted to resolve discrepancies through consensus. In the first phase, the title and abstract of each article were assessed to determine initial eligibility. Subsequently, articles that passed this initial screening underwent a meticulous review of the full text to ensure alignment with the predetermined inclusion criteria.
Data extraction
A data extraction sheet created using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) was made based on Cochrane Consumers and Communication Review Group’s data extraction template [16]. The process of extraction was independently performed by two reviewers (I.N. and V.P.). Any discrepancies during the extraction process were resolved through discussion and consensus between the reviewers. If consensus could not be reached, a third reviewer (I.M.) was consulted for adjudication.
The data extraction process from the included original articles encompassed two main categories: (i) participant information, which included details such as the number of participants, their age, competitive level, sex, randomisation procedures, study design, control intervention employed, tests utilised for assessment, and the specific outcome measures extracted. (ii) Gathering information on the characteristics of interventions, including those of the SSG intervention, as well as the active or control groups, was a key aspect of the studies. This included whether the intervention was combined with other methods of training, the duration of the intervention in weeks, the frequency of sessions (number of days per week), the total number of sessions, specifics regarding SSG formats utilised, such as pitch dimensions and any additional conditions imposed during the training sessions. Additionally, details on sets, repetitions, work duration, between repetition duration, and the type of recovery utilised were also collected.
Quality assessment
We utilised the Physiotherapy Evidence Database (PEDro) scale to evaluate the internal validity and risk of bias of the included studies [17]. This scale appraises the internal validity of studies, assigning scores ranging from 0 (indicating high risk of bias) to 10 (indicating low risk of bias). The scale encompasses eleven criteria, with criterion 1 excluded from the final score. Points for criteria 2 to 11 were allocated only when the criteria were met satisfactorily. Evaluation of articles was carried out independently by two authors (I.N. and V.P.), and disagreements were resolved through a consensus meeting or a rating by a third assessor (I.M.). In addition to the PEDro scale, Egger’s test for publication bias was conducted for the meta-analysis.
Summary measures
A meta-analysis was conducted when at least two study groups provided pre- and post-intervention data for the same measure [18]. Means and standard deviations for pre- and post-intervention measures (CODS) from SSG-based studies were used to compute Hedges’s g effect size (ES). The analyses for this meta-analysis were conducted using JASP (version 0.18.3, University of Amsterdam). These analyses included calculating ESs (Hedges’s g), applying a random-effects model, weighting studies by inverse variance, assessing heterogeneity using the Q statistic, tau-squared, H2, and I2, and evaluating publication bias using Egger’s test. The results are visually represented in a forest plot, summarising the ESs and their variability across the studies [19]. ESs were presented along with 95% confidence intervals (CIs) and interpreted using the following thresholds [20]: less than 0.2 is considered trivial, 0.2 to 0.6 is small, greater than 0.6 to 1.2 is moderate, greater than 1.2 to 2.0 is large, greater than 2.0 to 4.0 is very large, and greater than 4.0 is extremely large [12].
Results
Study selection
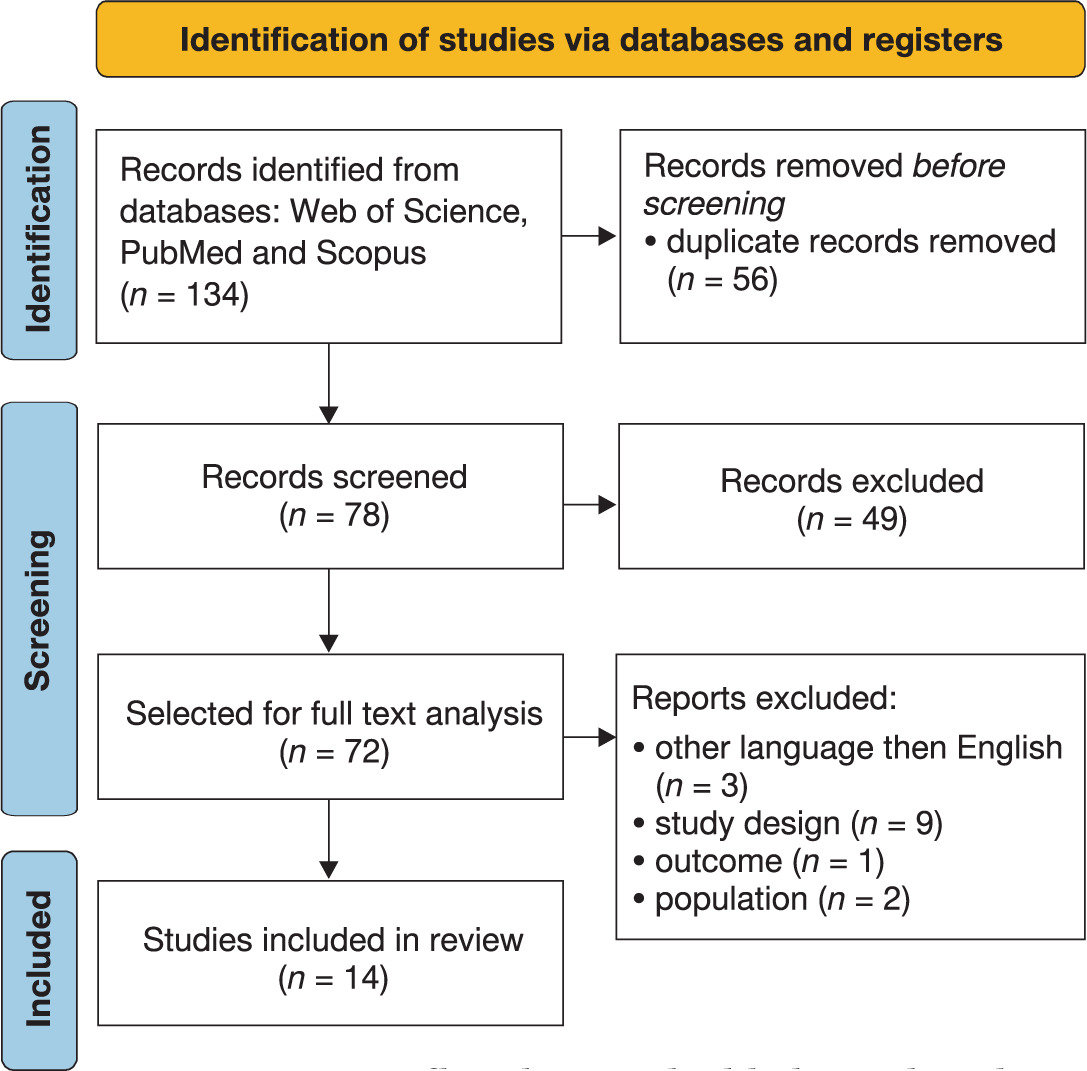
A total of 134 records were identified through searches in Web of Science (n = 66), PubMed (n = 41), and Scopus (n = 27), which were subsequently imported into the web application Rayyan for further analysis [21]. After removing duplicates, 78 unique records remained. These records underwent initial screening based on their titles and abstracts, resulting in the exclusion of 49 records that did not meet the predefined inclusion criteria. Subsequently, the full texts of the remaining 29 records were assessed for eligibility, leading to the exclusion of an additional 13 records because they were not written in English (n = 3), study design (e.g., non-parallel study, intervention duration less than 4 weeks, or lack of pre- and post-intervention data) (n = 9), other outcome extracted (n = 1), or included participants over 19 years old (n = 2). Ultimately, 14 studies were deemed eligible and included in the systematic review (Figure 1).
Study characteristics
The characteristics of the included studies are summarised in Table 1. Among the 14 studies included in this systematic review, all utilised a parallel study design. With the exception of one study focusing on futsal [22], the remaining studies centred on soccer. In terms of comparator groups for SSG interventions, the majority of studies employed running-based methods (RBMs) [22–29], other studies utilised regular football training [23, 30], and mixed approach between technical skill (TS) and a RBM [31, 32]. There were also SSGs combined with other running methods compared [33, 34] to simple SSG interventions [35] or regular football training [30].
Table 1
Summary of the study characteristics
| Study | Group: n | Age (years) mean ± SD | Level | Sex | Randomised | Study design | Control intervention | Tests used | outcome extracted |
|---|---|---|---|---|---|---|---|---|---|
| [23] | SSG: 12 COD: 12 CoN: 12 | 14.2 ± 0.9 | elite | M | yes | parallel | COD CoN: REG | COD 15 m 10-8-8-10 m zig-zag 20 m | CODS |
| [30] | SSG and HIT: 12 REG: 7 | 16.2 ± 0.8 | NM | M | yes | parallel | REG | L modified test | CODS |
| [31] | SSG: 12 SBT: 12 | 15.3 ± 3 | amateur | M | yes | parallel | SBT | T-test | CODS |
| [24] | SSG: 52 HVT: 50 | U16: 15.1 ± 0.3 U17: 15.9 ± 0.3 U19: 17.5 ± 0.5 | highly trained | NM | yes | parallel | HVT | K-test | CODS |
| [33] | SSG + sHIIT: 14 SSG + RST: 14 | 17.2 ± 0.4 | NM | NM | yes | parallel | no | 5-0-5 test | CODS |
| [25] | SSG: 12 HIIT: 12 | 18.63 ± 2.36 | NM | F | yes | parallel | HIIT | 5-0-5 test | CODS |
| [36] | SSG: 10 HIIT: 10 | 14.2 ± 0.5 | NM | M | NM | parallel | HIIT | zig-zag test | CODS |
| [37] | SSG: 12 HIIT: 12 | 16.7 ± 0.9 | NM | NM | yes | parallel | HIIT | modified T-test | CODS |
| [32] | SSG: 10 GPBT: 10 | 18.6 ± 0.6 | elite | M | yes | parallel | GPBT | RSA test | CODS |
| [22] | SSG: 12 GFT: 12 | 18.6 ± 0.5 | futsal | M | yes | parallel | GFT | arrowhead | CODS |
| [28] | SSG: 20 HIIT: 15 | 16.5 ± 0.5 | high level | NM | yes | parallel | HIIT | COD test | CODS |
| [29] | SSG: 20 HIIT: 20 | 16.4 ± 0.5 | regional | M | yes | parallel | HIIT | zig-zag test | CODS |
| [35] | SSG: 18 SSGC: 20 | 16.30 ± 0.47 | amateur | M | yes | parallel | no | zig-zag test | CODS |
| [34] | SSG + HIIT: 12 HIIT + SSG: 12 | 14.63 ± 0.71 | amateur | M | yes | parallel | no | zig-zag test | CODS |
[i] SSG – small sided games, COD – change of direction, CODS – change of direction speed, CoN – control group, HIT – running-based high intensity training group, REG – regular training, SBT – skill-based training at maximum intensity group, HVT – high volume running based training group, sHIIT – short high intensity interval training, RST – repeated sprint training, HIIT – running-based high intensity interval training group, GPBT – game profile–based training, GFT – generic fitness training, RAT – reactive agility test, SSGC – combined core strength and small-sided games, NM – not mentioned U16 – under 16 years old, U17 – under 17 years old, U19 – under 19 years old, M – male, F – female
Regarding participant demographics, nine studies involved male soccer players [22, 23, 29–32, 34–36], one study focused on females [25], and four did not specify the sex of the subjects [19, 23, 28, 32]. Following the level of participants, there were studies at the elite level [23, 32], amateur level [31, 34, 35], two at highly trained [24, 28], and five did not specify the level of players [25, 30, 33, 36, 37]. All included studies assessed CODS. The age of participants across the studies ranged from 9 to 19 years old.
The characteristics of SSG interventions are detailed in Table 2. The duration of training interventions varied across studies, with durations ranging from 4 weeks [24, 28–30, 33], 5 weeks [36], 6 weeks [22, 23, 34, 35, 37], to 8 weeks [25, 31, 32]. The formats of SSGs utilised varied from 1v1 to 6v6, with variations in game configuration, restrictions, and the presence or absence of coach encouragement.
Table 2
Characteristics of the SSG training interventions
| Study | Combination | Duration (weeks) | Days per week | Total sessions | Formats | Pitch dimensions | other condition | Sets | Reps | Work duration | Recovery duration | Type of recovery |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [23] | no | 6 | 3 | 18 | 1v1, 2v2, 3v3 | 10 × 20 20 × 20 20 × 30 | ball contacts restricted (2–3) | 2 | 2–4 | 30 s – 2 min | 2 min | NM |
| [30] | SSG and HIT | 4 | 4 | 16 | 4v4 | 30 × 25 | varied rules encourage | NM | 4 | 4 | 1 | passive |
| [31] | no | 8 | 2 | 16 | 3v3 | 20 × 25 | NM | NM | 4 | 6 | 2 | passive |
| [24] | no | 4 | 5 | 20 | 3v3, 4v4 | NM | NM | NM | 2–8 | 3–6 | 1–2 | NM |
| [33] | SSG + sHIIT | 4 | 2 | 8 | 2v2 | 20 × 25 | encourage | NM | 2 | 2 | 2 | NM |
| SSG + RST | 4 | 2 | 8 | 2v2 | 20 × 25 | encourage | NM | 2 | 2 | 2 | NM | |
| [25] | no | 8 | 3 | 24 | 2v2, 3v3 | 12 × 24 18 × 30 | encourage | 2 | 2 | 90 s | 90 s | NM |
| [36] | no | 5 | 2 | 10 | 2v2 pos 2v2 + gk 2v2 2v2 + 2 | 20 × 15 25 × 18 | NM | NM | 2 | 2.30– 4.30 | 2 | NM |
| [37] | no | 6 | 2 | 12 | 4v4 | 25 × 35 | NM | NM | 4 | 4 | 3 | passive |
| [32] | no | 8 | 2 | 16 | 5v5 + gk | 42 × 30 | encouragement | NM | 3–5 | 4 | 2 | passive |
| [22] | no | 6 | 3, 4 | 26 | 1v1 – 6v6 | 10 × 15–20 × 30 | NM | NM | 2–10 | 30 s – > 15 min | 30 s – 3 min | NM |
| [28] | no | 4 | 2 | 8 | 3v3 + gk 4v4 + gk | 35 × 25 40 × 30 | encourage | NM | 4 | 4 | 4 | passive |
| [29] | no | 4 | 3 | 12 | 2v2 + gk 2v2 pos | 20 × 18 20 × 15 | encourage | 2 | 2 | 2.30 – 4 | 2 | NM |
| [35] | no | 6 | 3 | 18 | 2v2 – 4v4 gk | 12 × 24–24 | encourage | NM | 4 | 2–4 | 3 | NM |
| SSGC | × 36 | |||||||||||
| [34] | SSG + HIIT | 6 | 2 | 12 | 2v2 – 4v4 | 15 × 27 20 × 30 25 × 32 | NM | 2 | 2–4 | 2–4 | 2 | NM |
| HIIT + SSG | 6 | 2 | 12 | 2v2 – 4v4 | 15 × 27 20 × 30 25 × 32 | NM | 2 | 2–4 | 2–4 | 2 | NM |
In Table 4, comprehensive details about the characteristics of the active or control group training programs in the studies are included. This information is crucial for understanding how SSG interventions compare to different training methods in terms of their impact on CODS and agility performance.
Risk of bias assessment
The PEDro scores for the 14 chosen articles varied from 5 to 9 out of a possible maximum of 10. No articles were omitted based on their scores. Concealment of allocation was not particularly pertinent in studies like these, given the context of football training and the methods of participant selection employed, it was challenging for researchers to maintain both their own and the participant’s unawareness of the treatment and group assignments. Blinding of subjects and therapists (i.e., trainers) was likewise not applicable in this instance [38].
After the quality assessment process, 3 studies obtain excellent methodological quality [32, 33, 37], 10 studies good methodological quality [22–25, 28–31, 34, 35], and one fair methodological quality [36]. The overall methodological quality of the intervention studies can be found in Table 3.
Results of individual studies
SSGs vs. RBMs on CODS performance
Table 5 provides a summary of the included studies and the results of CODS performance before and after interventions based on SSGs and RBMs. Eight studies provide data on CODS performance comparing SSGs and RBMs, with a total of 478 participants (n = 478).
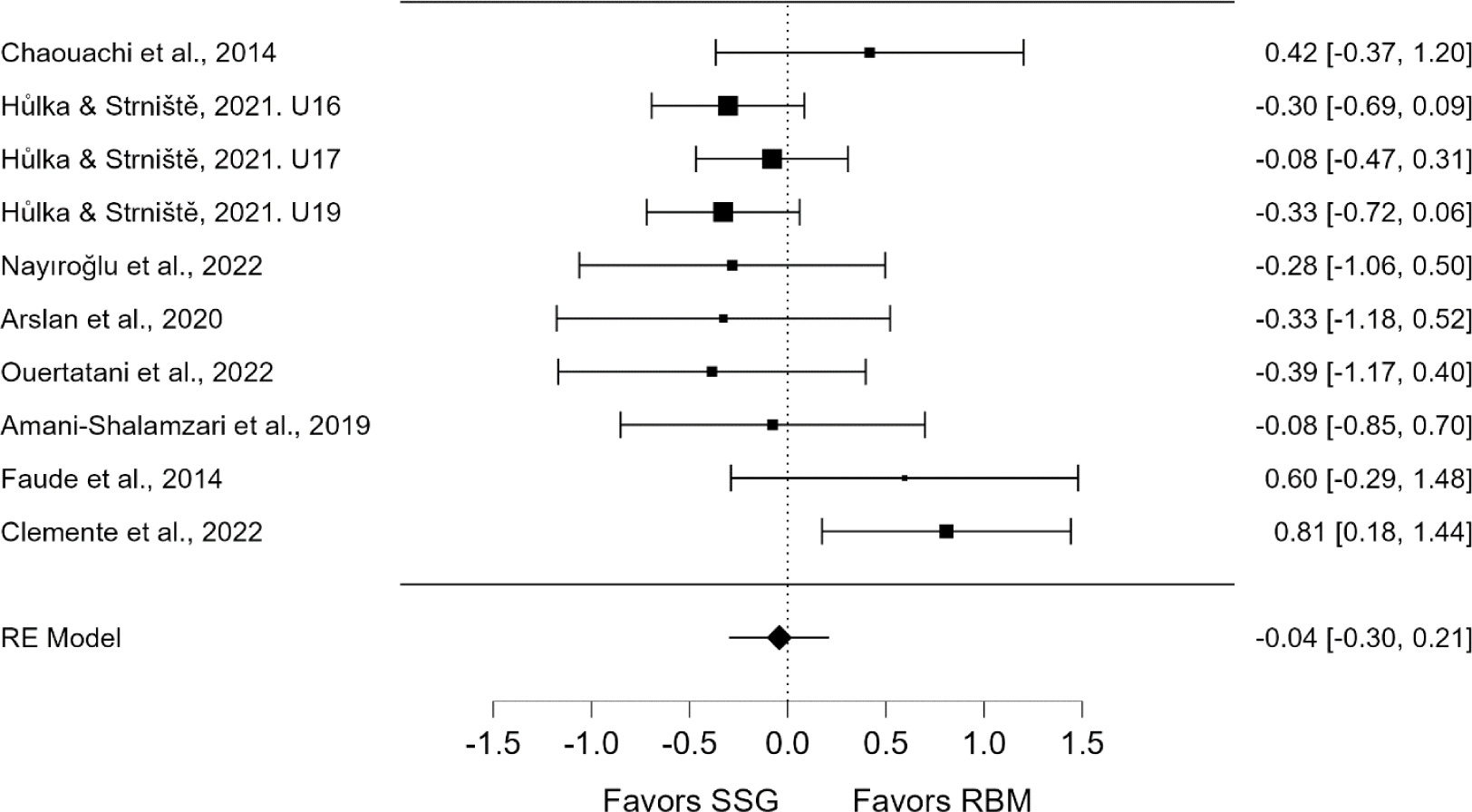
There was no significant difference between SSG-based and RBM interventions on CODS performance (ES = –0.04, 95% CI = –0.30 to 0.21, p = 0.74). The studies showed moderate heterogeneity (I2 = 43.17%, Q = 15.34, p = 0.082). The overall ES was not significant (z = –0.331, p = 0.74), suggesting no effect of SSGs versus RBMs. Additionally, Egger’s test showed no evidence of publication bias (p = 0.268). See Figure 2 for details.
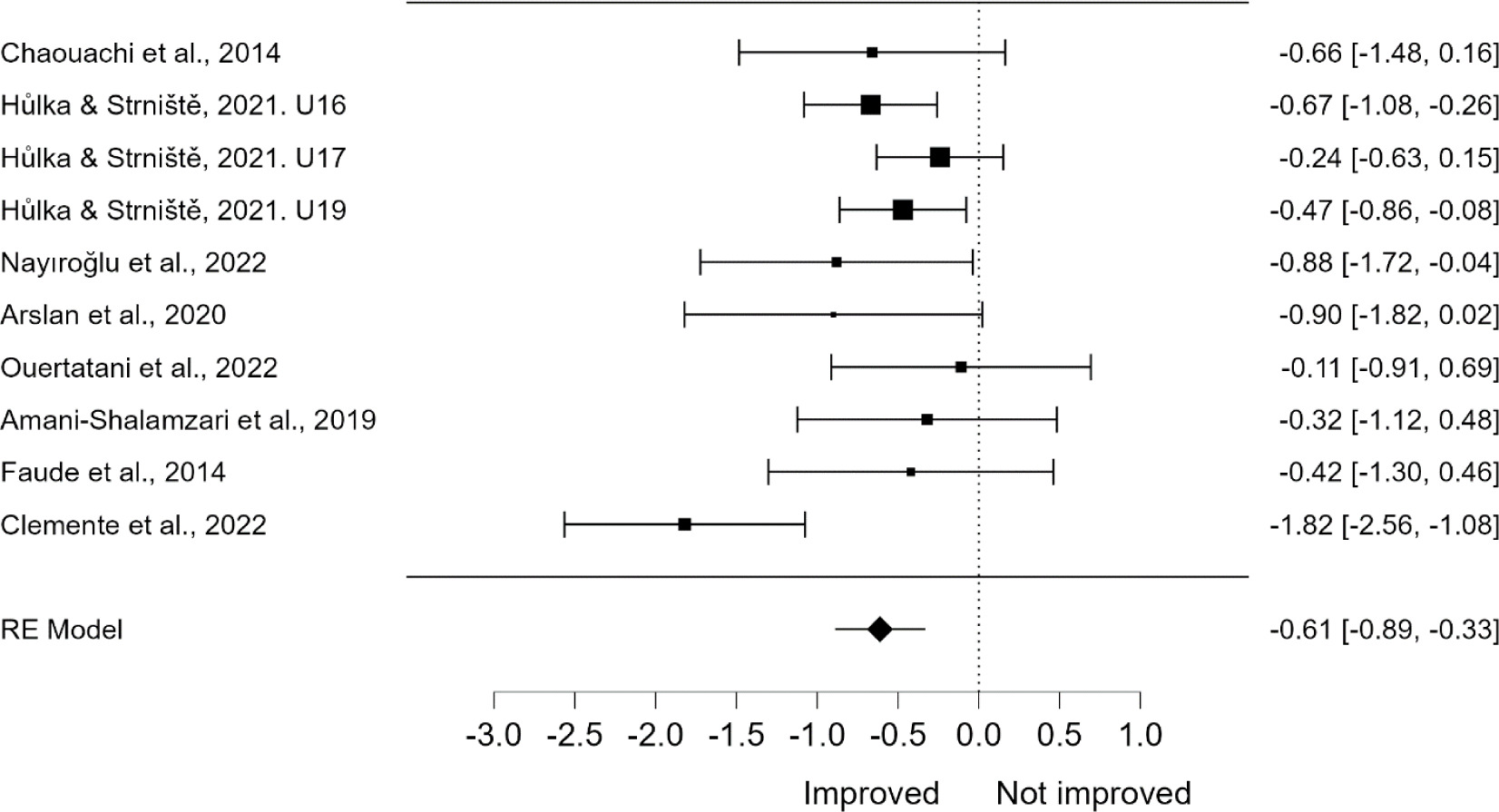
There was a significant improvement in CODS performance following RBM interventions (ES = –0.61, 95% CI = –0.89 to –0.33, p < 0.001). The studies showed moderate heterogeneity (I2 = 48.71%, Q = 16.81, p = 0.052), indicating some variability across studies. The overall ES (z = –4.27, p < 0.001) demonstrates that RBM interventions significantly improved performance. Egger’s test showed no evidence of publication bias (p = 0.420). See Figure 3 for details.
Table 3
Physiotherapy evidence database (PEDro) scale ratings
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [23] | y | y | n | y | n | n | n | y | y | y | y | 6 |
| [30] | y | y | n | y | n | n | n | y | y | y | y | 6 |
| [31] | y | y | n | y | n | n | n | y | y | y | y | 6 |
| [24] | y | y | n | y | n | n | n | y | y | y | y | 6 |
| [33] | y | y | n | y | y | y | y | y | y | y | y | 9 |
| [25] | y | y | n | y | n | n | n | y | y | y | y | 6 |
| [36] | y | n | n | y | n | n | n | y | y | y | y | 5 |
| [37] | y | y | n | y | y | y | y | y | y | y | y | 9 |
| [32] | y | y | n | y | y | y | y | y | y | y | y | 9 |
| [22] | y | y | n | y | n | n | n | y | y | y | y | 6 |
| [28] | y | y | n | y | n | n | n | y | y | y | y | 6 |
| [29] | y | y | n | y | n | n | n | y | y | y | y | 6 |
| [35] | y | y | n | y | n | n | n | y | y | y | y | 6 |
| [34] | y | y | n | y | n | n | n | y | y | y | y | 6 |
[i] PEDRro scale items – the total number of points from a possible maximal of 10, item 1 – eligibility criteria were specified, item 2 – subjects were randomly allocated to groups, item 3 – allocation was concealed, item 4 – the groups were similar at baseline regarding the most important prognostic indicators, item 5 – there was blinding of all subjects, item 6 – there was blinding of all therapists who administered the therapy, item 7 – there was blinding of all assessors who measured at least one key outcome, item 8 – measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups, item 9 – all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analysed by “intention to treat”, item 10 – the results of between-group statistical comparisons are reported for at least one key outcome, and item 11 – the study provides both point measures and measures of variability for at least one key outcome y – yes, n – no
Table 4
Characteristics of the active or control group training programs in the studies
| Study | Group | Characteristics |
|---|---|---|
| [23] | COD | The COD group engaged in structured COD exercises, which included preplanned drills such as skipping, the 5-0-5 m drill, the half-T-test over 20 m, and shuttle runs covering 4 sets of 10 m each. These drills did not involve the use of a ball. |
| CoN | The CoN players performed skill-development drills across all the training studies. | |
| [30] | SSG + HIT | One interval training session per week, layers performed 2 × 6 min (30/15 s) at 110% of 30–15 IFT test performance and 2 × 4 min (15/15 s) at 120% of 30–15 IFT test performance. The two sets were separated by a rest period of 90 s. The players performed 8 repetitions in each set. |
| REG | The REG group training included only 1 combined SSG and HIT session per week that consisted of 4 × 4 min SSG interspersed with 1-minute passive recovery and 2 × 6 min (30/15 s) at 110% 30–15 IFT test performance (8 repetitions in total). | |
| [31] | SBT | The training method employed various stations focusing on COD, shooting accuracy, and sprinting endurance. Stations included shuttle sprints with ball shooting, ball shooting around cones, and headshots followed by sprints. |
| [24] | HVT | The training sessions primarily targeted aerobic fitness with a structured format. Each session began with a 25-minute warm-up, followed by 25 min dedicated to football skills and tactics. The main segment of the session involved aerobic exercises such as fartlek and continuous running, with the remainder of the time allocated to a 10-minute cool-down period. |
| [33] | SSG + sHIIT | The short high-intensity interval training protocol included 2 sets of 5 repetitions, with each repetition consisting of 15 seconds of high-intensity work followed by 15 seconds of rest. During the work phase, participants exerted 90–95% of their individual maximal velocity attained during the IFT, while the rest phase was characterised by 0% of IFT intensity. |
| SSG + RST | The repeated sprint training protocol consisted of 2 sets of 4 repetitions, with each sprint covering a distance of 30 m. Participants rested for 20 s between sprints, maintaining work intensity at 100% effort while resting at 0% intensity. | |
| [25] | HIIT | The HIIT training protocol comprised 2–3 sets, each consisting of 6 repetitions. Each repetition involved 15 s of work followed by 15 s of rest, with a 4-minute rest period between sets at 65% of individual maximal velocity attained during the IFT. Work intensity was set at 90–95% of IFT, while rest intensity was maintained at 0% of IFT. |
| [36] | HIIT | The HIIT sessions, interval training without a soccer ball, consisted of intermittent running at 90–95% of players’ IFT for 15 s (around the pitch), followed by 15 s of passive recovery. |
| [37] | HIIT | Players alternated between running predetermined distances in 15-second intervals, followed by 15 s of passive rest. The distance covered was personalised based on each player’s maximal aerobic speed, set at 110% of their maximal aerobic speed. This cycle was repeated for four bouts, lasting 4 minutes each, with 3 min of passive rest between bouts. |
| [32] | GPBT | The GPBT protocol comprised 2–3 sets lasting 6–10 min each, integrating intermittent activities like walking, low to moderate running, high-intensity intermittent running, sprinting with COD, and passing drills, with an exercise intensity tailored to 50–75–105% of the maximal aerobic velocity achieved during the YYIRTL1. |
| [22] | GFT | The running regimen included jogging for recovery, running at various intensities (3–3.5 m/s) with diverse movements, alternating between 15-second intervals of high intensity (3.9–4.4 m/s) and low intensity, and sprinting at maximal intensity (> 5 m/s). |
| [28] | HIIT | The HIIT protocol involved two series of 12 to 15 repetitions of 15-second runs, with a rest-to-run ratio of 1:1 and a 10-minute rest between series. High-intensity runs were performed at 140% of IAT velocity, covering distances marked by cones ranging from 75 to 95 m. |
| [29] | HIIT | Participants completed two sessions of high-intensity interval training, each lasting 6 to 9 minutes, with intervals of 15 seconds of work followed by 15 s of rest, performed at 90% to 95% of their individual maximal velocity attained during the IFT. |
| [35] | SSGC | The SSGcore group engaged in a comprehensive core strength training regimen, comprising dynamic and static exercises such as push-ups, rotations, crunches, bird-dogs, scissor kicks, mountain climbers, and full squats, integrating seven popular upper and lower body movements, tailored to various small-sided game formats. |
| [34] | SSG + HIIT HIIT + SSG | Both groups followed two sets of protocols: HIIT, involving 2 × 5 min with 15-second intervals at 90% of IFT, alter nated with 15-second rest periods, and SSG, consisting of 2 sets of 2-minute small-sided games with 2 min of rest. However, the order of implementation varied, with one group starting with HIIT and the other with SSG. |
[i] COD – change of direction group, CON – control group, IFT – intermittent fitness test, REG – regular training group, SBT – skill-based training at maximum intensity group, HVT – high volume running-based training group, SSG – small-sided games, HIT – running-based high-intensity training group, sHIIT – short high-intensity interval training group, HIIT – running-based high-intensity interval training group, GPBT – game profile-based training group, YYIRTL1 – intermittent running test, GFT – generic fitness training group, IAT – individual anaerobic threshold, SSGC – combined core strength and small-sided games, RST – repeated sprint training,
Table 5
Summary of CODS performance following SSG and RBM interventions in youth soccer players
| Study | Group | Pre-intervention | Post-intervention | Pre-post ∆ % | ||
|---|---|---|---|---|---|---|
| mean | SD | mean | SD | |||
| [23] | SSG | 7.70 | 0.28 | 7.51 | 0.29 | –2.47 |
| [23] | COD | 7.40 | 0.56 | 7.03 | 0.47 | –5.00 |
| [24] | SSG U16 | 11.51 | 0.54 | 10.87 | 0.76 | –5.56 |
| [24] | HVT U16 | 11.74 | 0.64 | 11.30 | 0.65 | –3.75 |
| [24] | SSG U17 | 11.42 | 0.98 | 11.19 | 1.07 | –2.01 |
| [24] | HVT U17 | 11.25 | 0.52 | 11.09 | 0.78 | –1.42 |
| [24] | SSG U19 | 11.42 | 0.72 | 10.84 | 0.58 | –5.08 |
| [24] | HVT U19 | 11.32 | 0.79 | 10.97 | 0.67 | –3.09 |
| [25] | SSG | 2.72 | 0.11 | 2.59 | 0.09 | –4.78 |
| [25] | HIIT | 2.87 | 0.10 | 2.77 | 0.11 | –3.48 |
| [36] | SSG | 6.92 | 0.19 | 6.68 | 0.15 | –3.47 |
| [36] | HIIT | 7.09 | 0.20 | 6.91 | 0.16 | –2.54 |
| [37] | SSG | 5.87 | 0.26 | 5.72 | 0.17 | –2.56 |
| [37] | HIIT | 5.92 | 0.40 | 5.88 | 0.22 | –0.68 |
| [22] | SSG | 15.35 | 0.51 | 15.13 | 0.48 | –1.43 |
| [22] | GFT | 15.28 | 0.55 | 15.10 | 0.48 | –1.18 |
| [28] | SSG | 7.85 | 0.22 | 7.88 | 0.26 | 0.38 |
| [28] | HIIT | 7.90 | 0.30 | 7.74 | 0.39 | –2.03 |
| [29] | SSG | 5.59 | 0.29 | 5.40 | 0.22 | –3.40 |
| [29] | HIIT | 5.62 | 0.21 | 5.24 | 0.19 | –6.76 |
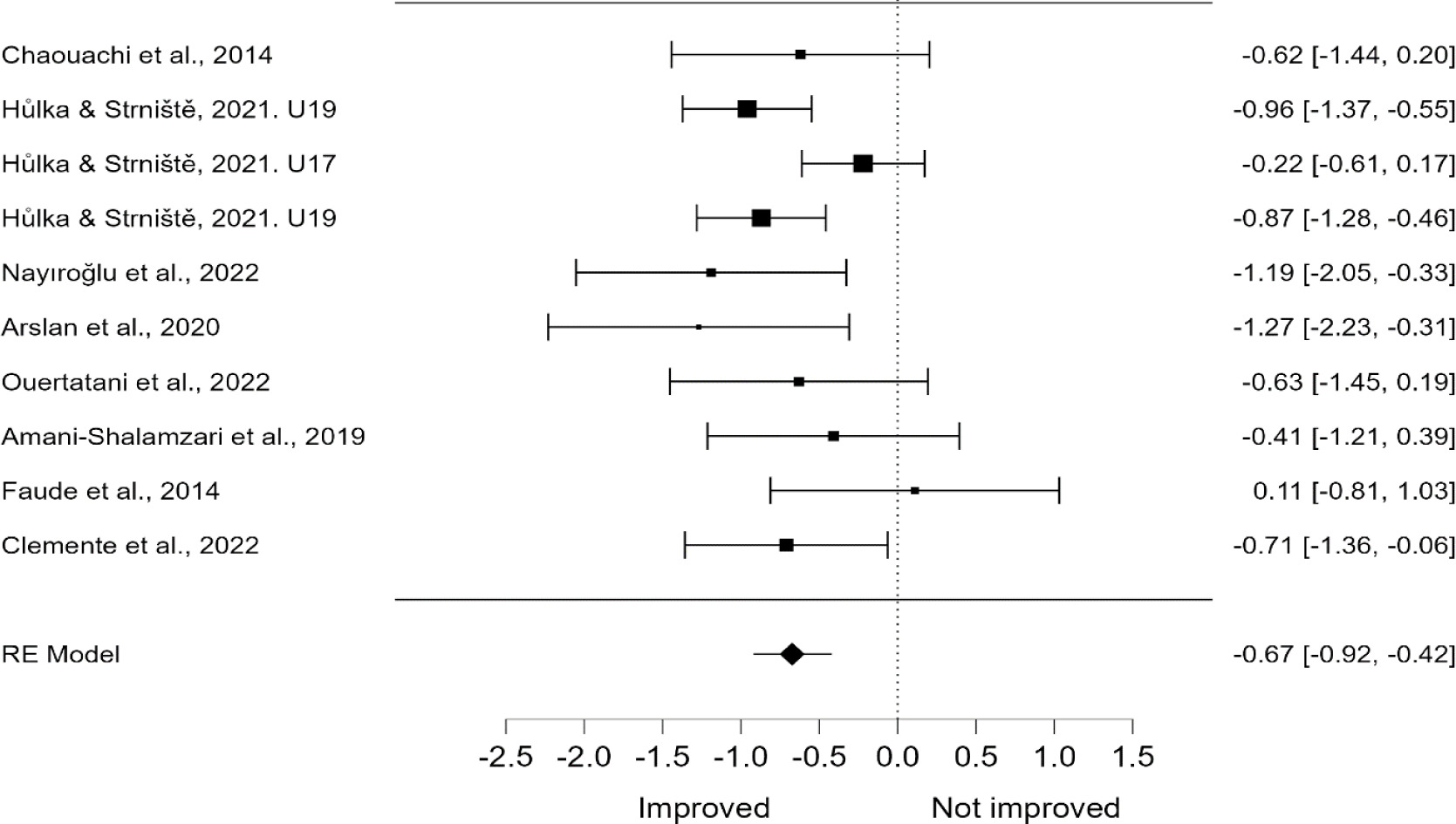
There was a significant improvement in CODS performance following SSG interventions (ES = –0.67, 95% CI = –0.92 to –0.42, p < 0.001). Heterogeneity was moderate (I2 = 35.92%), indicating variability across studies, however, the test of residual heterogeneity was not significant (Q = 13.967, p = 0.124). The overall ES (z = –5.277, p < 0.001) shows SSG interventions significantly improve CODS times (see Figure 4). Egger’s test found no evidence of publication bias (p = 0.951).
SSGs vs TS and RBMs on CODS performance
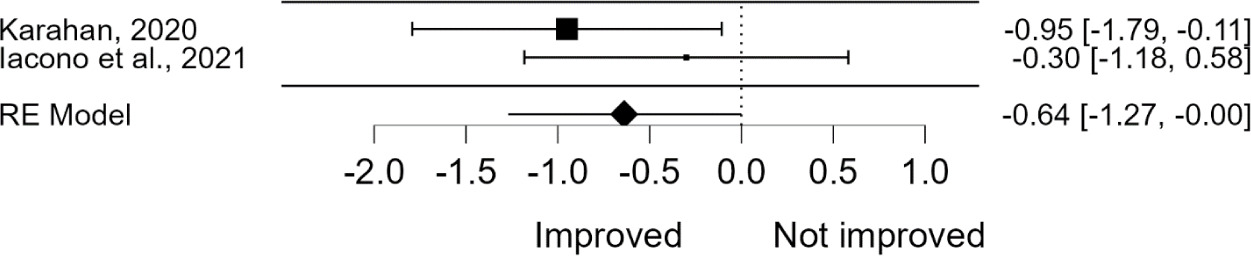
Table 6 provides a summary of the included studies and the results of CODS performances before and after interventions based on SSGs and TS and RBMs. Two studies provided data on CODS performance comparing SSGs and TS and RBMs, with a total of 44 participants (n = 44).
There was no significant difference between SSG-based and TS and RBM interventions in CODS performance (ES = –0.84, 95% CI = –3.72 to 2.04, p = 0.568). Heterogeneity was very high (I2 = 94.09%), indicating that most of the variability in ESs is due to differences across studies. The test of residual heterogeneity was significant (Q = 16.926, df = 1, p < 0.001). The overall test of ES was not significant (z = –0.571, p = 0.568), suggesting no clear advantage of SSGs over TS and RBMs for improving CODS performance (see Figure 5).
Within-group SSG analyses were not performed here due to the limited number of available studies. However, the impact of SSGs within groups has been thoroughly assessed in the SSGs vs RBMs section, where a larger number of studies were included.
There was a significant improvement in CODS performance following the TS and RBM interventions (ES = –0.64, 95% CI = –1.27 to –0.00, p = 0.049). The relative weight of each study in the analysis ranged from 50.94% to 49.06%. The heterogeneity among the studies was low (I2 = 8.31%), indicating that only a small portion of the variability in ESs is due to differences across the studies. The test for residual heterogeneity was not significant (Q = 1.091, df = 1, p = 0.296), suggesting that the variability across studies is primarily due to chance. The overall test of ES (z = –1.966, p = 0.049) shows a significant reduction in CODS times, indicating that TS and RBM interventions lead to improved performance (see Figure 6).
Table 6
Summary of CODS performance following SSG and TS and RBM interventions in youth soccer players
| Study | Group | Pre-intervention | Post-intervention | Pre-post ∆ % | ||
|---|---|---|---|---|---|---|
| mean | SD | mean | SD | |||
| [31] | SSG | 10.9 | 0.4 | 10.74 | 0.4 | –1.47 |
| [31] | SBT | 11.1 | 0.4 | 10.69 | 0.4 | –3.69 |
| [32] | SSG | 1.18 | 0.03 | 1.09 | 0.04 | –7.63 |
| [32] | GPBT | 1.19 | 0.03 | 1.18 | 0.03 | –0.84 |
Table 7
Summary of CODS performance following combination SSG interventions in youth soccer players
| Study | Group | Pre-intervention | Post-intervention | Pre-post ∆ % | ||
|---|---|---|---|---|---|---|
| mean | SD | mean | SD | |||
| [30] | SSG and HIT r | 4.21 | 0.1 | 4.08 | 0.2 | –3.1 |
| [30] | REG r | 3.89 | 0.1 | 3.88 | 0.1 | –0.3 |
| [30] | SSG and HIT l | 4.23 | 0.2 | 4.16 | 0.1 | –1.7 |
| [30] | REG l | 3.91 | 0.1 | 3.88 | 0.1 | –0.8 |
| [33] | SSG and sHIIT | 3.98 | 0.29 | 3.84 | 0.29 | –3.5 |
| [33] | SSG and RST | 4.04 | 0.21 | 3.79 | 0.26 | –6.2 |
| [35] | SSGcore | 5.98 | 0.23 | 5.5 | 0.36 | –8.0 |
| [35] | SSG | 5.86 | 0.19 | 5.53 | 0.23 | –5.6 |
| [34] | SSG and HIIT | 6.92 | 0.23 | 6.79 | 0.23 | –1.9 |
| [34] | HIIT and SSG | 6.79 | 0.36 | 6.66 | 0.37 | –1.9 |
[i] SSG – small-sided games, HIT (r/l) – high-intensity training (right/left leg tested), REG (r/l) – regular training (right/left leg tested), sHIIT – short high-intensity interval training, RST – repeated sprint training, SSGcore – combined core strength and small-sided games, HIIT – running-based high-intensity interval training

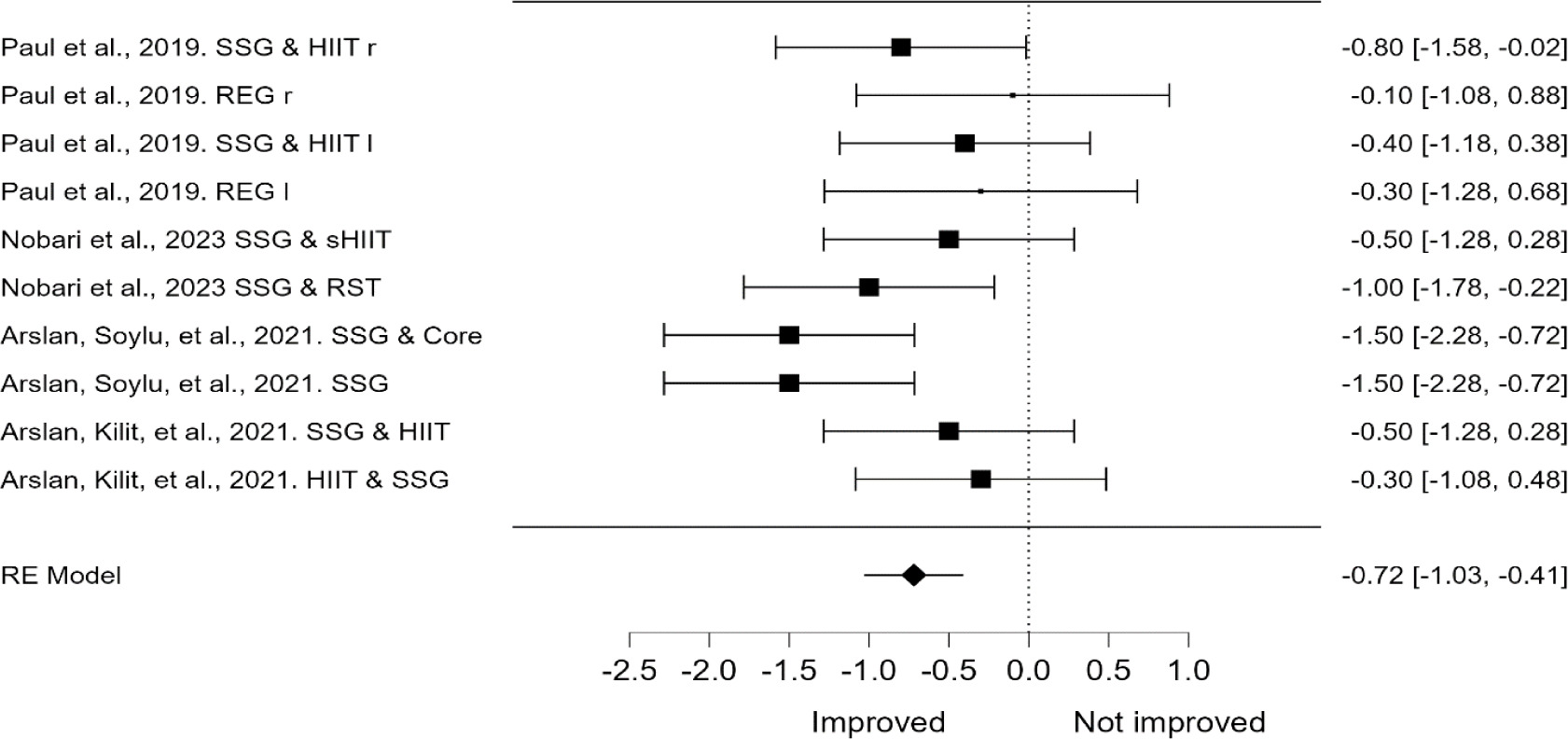
Combination of SSG effects on CODS performance
Table 7 provides a summary of the included studies and the results of CODS performances before and after interventions based on combining SSGs with other training methods and simply SSGs or regular football training, including four studies, with a total of 109 participants (n = 109).
In this meta-analysis, only within-group ESs were calculated, including combinations of SSG with other training methods (based on running and on core strength), because the active control groups also included diverse SSGs or combined interventions.
The combination of SSG interventions significantly improved CODS performance (ES = –0.72, 95% CI = –1.03 to –0.41, p < 0.001). Heterogeneity was moderate (I2 = 29.42%), with variability largely due to chance (Q = 12.722, p = 0.176). The overall ES (z = –4.586, p < 0.001) suggests that combining SSG with other training methods significantly reduces CODS times, with no evidence of publication bias (Egger’s test p = 0.145, see Figure 7).
Discussion
The findings of this systematic review shed light on the comparative effectiveness of SSG interventions versus various training methods on CODS performance. There are three main topics of discussion (i) SSG vs RBM, (ii) SSG vs TS and RBM, and (iii) analysing the efficacy of SSG combinations with RBM and core strength on CODS performance.
SSG compared with RBM on CODS performance
While there were no significant differences between SSG and RBM in the between-group comparisons, within-group analyses show that both interventions significantly improved CODS performance, with a slight advantage for SSG. our study partially aligns with Clemente et al. [39], which stated that there is no significant difference between SSG and RBM HIIT in team sports. However, our results indicate that the intra-group ES is slightly better for SSG compared to RBM, while they observed the opposite. It is important to note that they used only HIIT interventions, whereas we also included HVT and COD interventions in our grouping. Therefore, this comparison must be treated with caution.
The advantage of SSG compared with HVT or HIIT can be attributed to the nature of the game, meaning that during the game, the players execute an increased number of CODs compared with HVT or HIIT, which uses linear running at high intensity. There is also a study included in this subgroup that shows a much better advantage for COD interventions compared with SSG [23]. Based on these findings, we conclude the importance of training specific movements, in our case, CODS.
SSG Compared with TS and RBM on CODS performance
Our analysis revealed no significant difference between SSG-based and TS and RBM interventions due to the high heterogeneity. In contrast, groups receiving only TS and RBM interventions showed a marginally significant improvement. To our knowledge, there is no other systematic review or meta-analysis comparing the relationship between these two methods.
The heterogeneity can be attributed primarily to the limited number of studies (two) included in the analysis and the differences in their results. Although the literature on TS and RBM in comparison to SSG is limited, the differences observed between our included studies – Iacono et al. [32] and Karahan [31] — may be due to factors such as the age of participants, level of manifestation, and the tests used for measuring CODS. Additionally, variations in the format of the SSG intervention may contribute to the heterogeneity, whereas the TS and RBM protocols remained more consistent across studies.
Eficacity of SSG combinations with other training interventions
The statistical analyses show significant and robust improvements in CODS performance with combined SSG interventions. However, another systematic review by [40], including both youth and adults, found that SSG interventions combined and alone do not have a meaningfully beneficial impact on CODS performance.
Firstly, most studies in this SR included a combination of SSG and RBM with HIIT or RST. HIIT aims to improve the aerobic system, with some anaerobic involvement and muscle strain. RST, on the other hand, focuses more on the anaerobic system and stresses the movement system [33, 41], showing better improvement than HIIT, possibly due to greater neuromuscular strain [33]. Another reason for combining SSG with other methods is that SSGs alone reduce players’ exposure to high-intensity running (e.g., above 19.8 km/h) due to the small pitch size [42, 43].
Additionally, combining core strength training with SSGs brings significant positive results to CODS performance. It is known that core strength training in young soccer players improves sport-specific performances, including balance [44], endurance [45], and agility [46]. Yet no significantly big differences between SSGC and simple SSG [35].
Limitations of the review processes
While conducting this systematic review, we acknowledge several limitations in our review processes. First, our search was restricted to studies published in English, potentially omitting valuable research published in other languages. Secondly, access to only three databases may have limited the scope of our search and resulted in overlooking relevant studies. Additionally, the included studies exhibited heterogeneity in terms of methodologies, interventions, and outcome measures, making it challenging to directly compare results across studies. Despite these limitations, our review provides valuable insights into the comparative effectiveness of SSG interventions versus various training methods on CODS performance.
Study limitations
One limitation of this SRMA is the inherent differences in study characteristics. These differences arise from variations in intervention design, duration, SSG formats, and intensity, all of which can impact the effectiveness of SSG interventions and other training methods. Additionally, the limited number of studies comparing SSG versus TS and RBM, as well as those comparing SSG combined with other training methods against other training methods, represents a significant limitation. This scarcity restricts the ability to generalise the findings and underscores the need for further research to explore these training combinations in more depth.
Moreover, the majority of studies included male participants, with only one study focusing on females and several not specifying the sex of the subjects. This gender imbalance limits the applicability of the findings across different populations. Additionally, the participant levels varied widely, from elite to amateur, which may influence the training outcomes and should be considered when interpreting the results.
Finally, the methodological quality of the included studies varied, with most studies rated as having a good methodological quality, but some only achieving fair quality. This variation in study quality may affect the robustness of the conclusions drawn from this SRMA.
Future research
Given the inherent differences in study characteristics included in this review, future research should aim to standardise intervention designs, durations, SSG formats, and intensities to better compare the effectiveness of SSG interventions and other training modalities. More studies are needed to compare SSG versus TS and RBM and to examine the efficacy of SSG combined with other training methods against other training methods. Additionally, future research should include a more balanced representation of male and female participants and specify participant characteristics such as age and training level to enhance the generalizability of the findings.
Further investigation is also required to explore the mechanisms behind the observed improvements in CODS with combined SSG interventions. Specifically, research should examine how different combinations of training methods (e.g., SSG with HIIT, RST, or core strength training) impact neuromuscular and physiological adaptations in athletes. This could provide insights into optimising training regimens for various sports and performance outcomes.
Practical applications
The results of this review suggest that incorporating SSGs into training programs can significantly improve CODS, especially when combined with other training methods such as HIIT, RST, or core strength training. Coaches and practitioners should consider integrating these combined approaches to enhance both aerobic and anaerobic capacities, as well as overall agility and performance in athletes.
However, it is important to tailor training programs to the specific needs and characteristics of the athlete, taking into account factors such as age, gender, and training level. For instance, while SSGs alone may reduce high-intensity running exposure due to the small pitch size, combining SSGs with RBMs can address this limitation and provide a more comprehensive training stimulus.
Conclusions
This SRMA highlighted the effectiveness of SSG interventions compared to various training methods on CODS performance. SSGs and RBMs significantly improved CODS within groups, with a slight advantage for SSGs. However, the comparison between SSG and TS and RBM revealed no significant difference due to high heterogeneity, although TS and RBM showed marginally significant improvements. Combined SSG interventions demonstrated robust improvements in CODS performance, indicating their potential effectiveness in youth soccer players.
The study faced limitations due to the inherent variability and heterogeneity across the included studies, differences in intervention design, duration, format, and intensity, and the limited number of studies comparing SSGs with TS and RBMs and other methods. Additionally, the majority of studies included male participants, which limits the generalizability of the findings. The methodological quality of the studies varied, potentially affecting the robustness of the conclusions.
Future research should standardise intervention designs, durations, SSG formats, and intensities to facilitate better comparisons and include a balanced representation of genders and participant characteristics. Investigating the mechanisms behind CODS improvements with combined SSG interventions can provide further insights. Practically, coaches should integrate SSGs with HIIT, RST, or core strength training to enhance CODS and overall athletic performances, tailoring programs to the specific needs of athletes, considering factors such as age, gender, and training level.