Introduction
Cardiorespiratory fitness has a significant impact on human life expectancy and strongly determines the ability to perform aerobic exercise [1]. The gold standard for exercise assessment of cardiorespiratory fitness is maximal oxygen uptake (VO2max) [2]. Systematically performed training can improve VO2max [3]. The available literature compares the effectiveness of high-intensity interval training (HIIT), low-intensity training (LIT), and moderate-intensity training (MIT) (close to the level of lactate threshold or second ventilatory threshold) in improving cardiorespiratory fitness, as assessed by VO2max measurement [4]. It has been shown that HIIT is one of the most effective means of improving cardiorespiratory function and, in turn, physical performance [5–7]. Buchheit and Laursen [6] described four HIIT formats: long interval HIIT, short interval HIItT sprint interval training (SIT), and repeated sprint training (RST). The formats of HIIT differ in the intensity and duration of exercise, intensity, and duration of recovery periods, exercise modality, number of repetitions, number of sets, as well as the between-sets recovery duration and intensity [4, 6, 8].
Some authors assess changes in cardiorespiratory fitness as a result of a program focused solely on one form of training: SIT, HIIT or LIT [4, 9, 10]. Others, in turn, evaluate the impact of training programs incorporating several forms of training, with one example being a polarised training program (POL) [11, 12]. It is described as a training cycle characterised by polarisation of the training intensity and incorporates low-intensity training as well as high-intensity training [11, 12]. The volume of low-intensity training sessions is approximately 80% of the total training volume, while the high-intensity training is approximately 20% of the total training volume [11–13]. In polarised training programs, moderate-intensity training at the level of the lactate threshold or the second ventilatory threshold (VT2) is not used [7, 13], or these training sessions account for a small part of the training program (up to 5–10% of the total training volume) [14]. Some authors showed that a polarised training program induced greater improvements in aerobic capacity among athletes compared to a program consisting of LIT and MIT [15, 16] and compared to a program focused solely on LIT, a program focused solely on MIT, or a program focused solely on HIIT [12]. The available literature lacks information on the effects of a polarised training program consisting of two HIIT formats (long interval HIIT and SIT) and LIT on cardiorespiratory fitness among active, but non-athlete individuals.
However, cardiovascular fitness can be compromised, for example, by arteriosclerosis [17]. Arteriosclerosis causes narrowing of the lumen of blood vessels, leading to reduced blood flow, resulting in tissue hypoxia [17, 18]. The development of arteriosclerosis is associated, among other things, with the oxidation of low-density lipoproteins (LDL) under oxidative stress, leading to the formation of the oxidised form of LDL (ox-LDL) [18, 19]. Then, ox-LDL can be attached, for example, to the lectin-like oxidised low-density lipo-protein receptor-1 (LOX-1) within macrophages and vascular smooth muscle cells, contributing to the formation of foam cells [17, 19]. LOX-1 expression can be increased by proatherogenic factors [17]. It is believed that regular physical exercise reduces the risk of arteriosclerosis [17]. The individuals characterised by low VO2max were also characterised by an unfavourable lipid profile [18]. It has been shown that regular physical activity decreases the ox-LDL concentration [20]. However, this effect occurred only in the group with the highest training load, in which moderate- and high-intensity training was performed at least three times a week [20]. In turn, in groups in which low- or moderate-intensity training was performed less than three times a week, there was no decrease in ox-LDL concentration [20]. On the other hand, a high training load may be a factor that increases the risk of coronary arteriosclerosis of the carotid and peripheral arteries [21]. Atherosclerotic plaques were observed in the carotid and peripheral arteries in a group of marathon runners aged 45–75 years, performing high- and moderate-intensity training lasting 2–4 hours every day [21, 22]. The literature lacks information on changes in the concentration of ox-LDL and LOX-1 in the blood as a result of performing a polarised training program that combines low- and high-intensity training, therefore, this became the aim of the presented study.
This study aimed to assess the impact of four distinct training programs on maximal oxygen uptake and cardiovascular health markers, such as serum LOX-1 and ox-LDL concentrations. The programs included: 1) a polarised training program (POL) incorporating SIT, HIIT with long intervals, and LIT; 2) a program focused solely on SIT; 3) a program focused solely on long interval HIIT; and 4) a program focused solely on LIT. We hypothesised that POL would produce better results in these aspects than programs consisting of one-format training sessions.
Materials and methods
Participants and study design
Forty physically active individuals took part in the randomised controlled trial. Each of the participants undertook recreational physical activity at least twice a week, for a total time of at least 2–3 hours each week. The level of physical activity was characterised based on an interview with the individuals recruited for the experiment. None of the participants trained as an athlete or participated in any sports competition. All participants were non-smokers and did not use drugs. Participants were divided into four groups: group POL (n = 10, including 8 men and 2 women), group SIT (n = 10, including 7 men and 3 women), group HIIT (n = 10, including 7 men and 3 women), and group LIT (n = 10, including 7 men and 3 women).
The division into groups was made using block randomisation. The participants were divided into four-person blocks. Each block included participants with a similar VO2max value. Then, from each block, one participant was randomly assigned to each training group. The block randomisation method was intended to minimise the impact of the participants’ initial physical fitness on the study results. To assess the risk of bias, the ROB2 software for randomised clinical trials was used. The assessment was carried out in six areas (randomisation process, timing of identification or recruitment of participants, deviations of intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result). A low level of risk of biased judgement was obtained in each area. During the experiment, each group performed a different training program: group POL, group SIT, group HIIT, and group LIT. A detailed description of the training programs can be found below in the training intervention section.
Immediately before performing laboratory exercise tests (both before and after the training intervention), immunoenzymatic tests were performed to detect IgM and IgG antibodies against the receptor-binding domain – the S1 subunit of the S protein of the SARSCoV-2 virus (TestLine Clinical Diagnostics, Brno, Czech republic) in blood serum samples. The tests were performed before the vaccination campaign began, so the participants could not have antibodies that appeared after receiving the vaccination. Positive results of IgM (above 16 U ml–1) obtained immediately before the laboratory exercise tests were treated as a sign of infection and were the reason for exclusion from the study. Positive results of IgG (above 16 U ml–1) obtained immediately before the laboratory exercise tests performed after the training intervention were considered evidence of infection during the experiment, and such a participant was excluded from the study. Participants excluded from the study were replaced by newly recruited individuals. Participants were selected so that the groups consisted of a similar number of men and women (only in the POL group there was one woman less than in the other groups). The anthropo-metric and physiological characteristics of the groups are shown in Table 1.
Table 1.
Anthropometric and physiological characteristics of groups
Test procedures
Each participant underwent laboratory tests before and after the experiment, which included a resting venous blood sample and incremental step test – done on one day, and a test verifying the level of maximal oxygen uptake (VO2max verification phase) – done on a subsequent day. During the 48 hours preceding the incremental step test, participants did not perform any exercise or training. Each of the performance tests was performed in controlled laboratory conditions (temperature 20°C and humidity 45–50%).
Collection and labelling of blood samples
A 5 ml blood sample was collected from a vein at the elbow bend of each participant. Blood samples were taken 30 minutes before the incremental test, and at least 150 minutes after eating a standardised carbohydrate meal. Blood samples were collected in Sarstedt tubes with serous granules (Stamar, Poland) and then allowed to clot at room temperature for 30 min. the samples were then centrifuged for 10 min at 3000 rpm (Eppendorf Centrifuge 5810, Hamburg, Germany). Serum was extracted and then stored in Eppendorf tubes at –80°C. Following all blood collections, analyses of the ox-LDL and (LOX-1) concentrations were performed. After thawing, the samples were analysed by ELISA. Marking was performed using immunoenzymatic assay kits for ox-LDL (Wuhan Fine Biotech Co. Ltd., Wuhan, China) and LOX-1 (Wuhan Fine Biotech Co. Ltd., Wuhan, China).
Incremental Step test
The incremental step test was performed on a Lode Excalibur Sport cycle ergometer (Lode BV, Groningen, the Netherlands). The test consisted of several 3-minute steps. During each step, the effort was performed with constant intensity – power. When 3 minutes elapsed, the power was increased. The starting workload was 50 W for men and 40 W for women and increased every 3 min by 50 W for men and 40 W for women until volitional exhaustion was reached. For example, for men 50 W 100 W 150 W 200 W, etc., for women 40 W 80 W 120 W 160 W, etc. the duration of the incremental test may affect the VO2 peak value [23, 24]. Therefore, different power increments were used among men and women. This approach reduces the differences in test duration between men and women [23, 24]. Time and instantaneous power output were continually recorded. If the participant was unable to complete the last 3-minute step, then 0.28 W for men and 0.22 W for women was subtracted for each missing second from the current level of power. In this way, maximal aerobic power (Pmax) was calculated [16, 25].
During the incremental step test, the respiratory function was measured using a Quark CPET analyser (Cosmed, rome, Italy), which was calibrated before each test with a reference gas mixture of carbon dioxide (5%), oxygen (16%), and nitrogen (79%). tidal volume was analysed on a breath-by-breath basis to determine the oxygen uptake (VO2), volume of carbon dioxide expired (VCO2) and volume of air breathed per minute (VE). The absolute and relative (per kg of body mass) VO2 peak was calculated based on the data averaged over 30-s intervals. Based on the respiratory data records from the incremental test, the first ventilatory threshold (VT1) was determined at the point preceding the first non-linear increase in volume of air breathed per minute per volume of oxygen consumed (VE VO2–1) without a concomitant increase in volume of air breathed per minute per volume of carbon dioxide expired (VE VCO2–1) equivalent [24]. The second ventilatory threshold (Vt2) was at the point preceding the second non-linear increase in VE VO2–1 accompanied by an increase of VE VCO2–1 equivalent [24]. The heart rate (HR) was recorded using a Polar H10 sensor (Polar Electro Oy, tempele, Finland).
VO2max verification phase
The verification phase was preceded by a warm-up consisting of five 5-minute exercises at an intensity corresponding to the power achieved at VT1, then 10 min at a power corresponding to half the distance between the VT1 and the VT2. the warm-up was followed by a 10-minute passive break. A load of 110% Pmax was applied during the verification phase. The verification phase used the same procedures for measuring respiratory parameters as the incremental step test. The higher VO2 peak value (of those measured in the incremental step test and the verification phase) was defined as the maximal oxygen uptake (VO2max). Using the same principle, maximal values for volume of air breathed per minute (VEmax) and heart rate (HRmax) were indicated. Maximal exercise respiratory rate (RERmax) was determined based on data collected in an incremental step test.
Training interventions
During the 5-week experiment, participants in each study group performed 3 training sessions per week, each training session lasting approx. 45–50 min (1st–2nd week) and approx. 60–65 min (3rd–5th week). The course of the experiment is shown in Figure 1. The POL group performed a polarised training program consisting of SIT, long interval HIIT, and LIT. The SIT group performed a program focused solely on SIT; the HIIT group performed a program focused solely on long interval HIIT; and the LIT group performed a program focused solely on LIT. All training sessions were performed on a Monark LT2 cycle ergometer (Monark, Varberg, Sweden), and are described below:
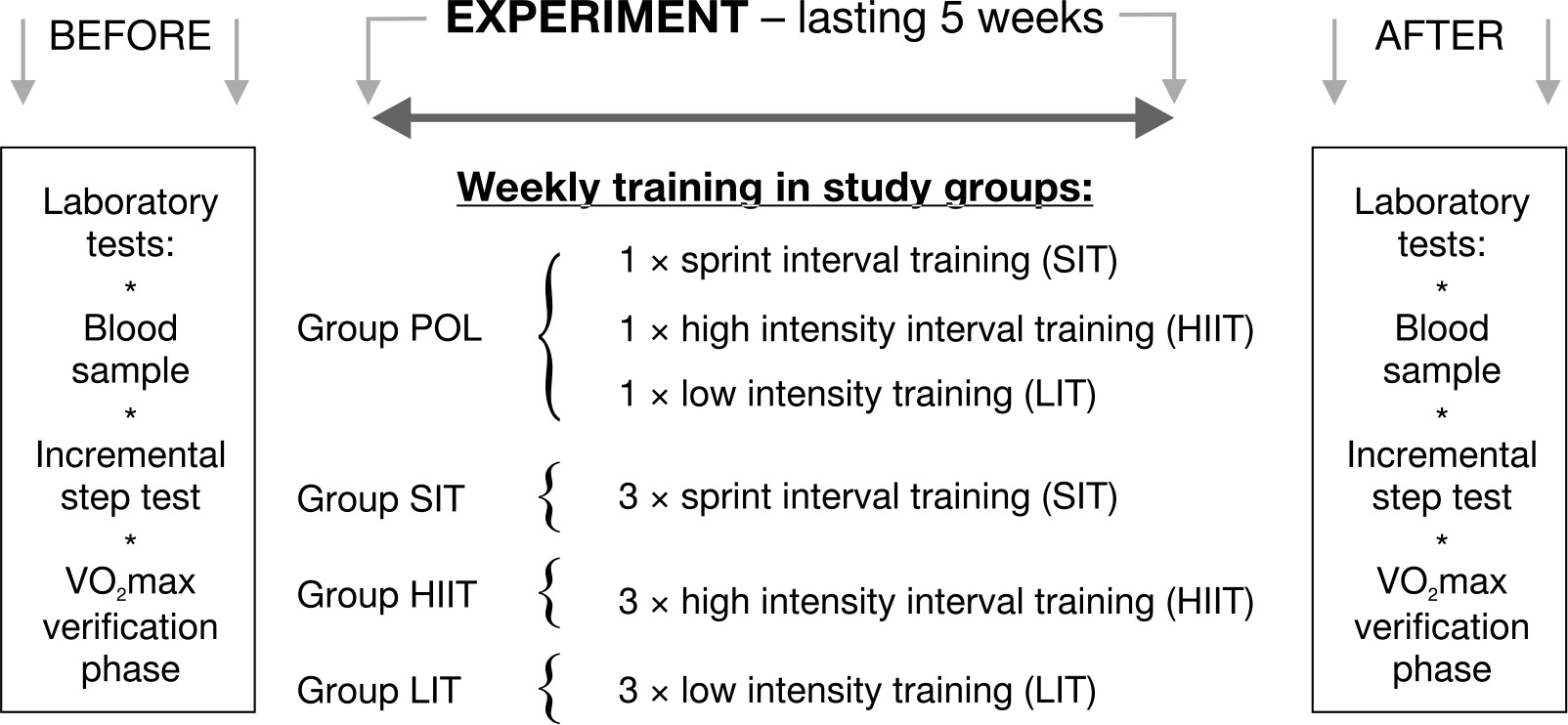
Sprint interval training (SIT), consisting of 6–10 repetitions at maximal intensity (all-out effort at a torque factor of 0.7 Nm · kg–1) lasting 30 s. the training session comprised two sets, with 3–5 maximal repetitions executed in each set. Active rest intervals of 90 seconds separated repetitions, during which participants engaged in exercise at a power not exceeding 25 W. Between the sets, a 15-minute active rest period was implemented, during which exercise was conducted at the power level reached at VT1, as determined in the incremental step test. In the initial phase of the experiment (1st–2nd week), all participants completed 6 repetitions during SIT. Subsequently, in the later weeks of the experiment (3rd–5th week), the participants increased the number of repetitions to 10 during SIT.
High-intensity interval training (HIIT) with long intervals, consisting of 4–5 bouts lasting 3 min and performed at an intensity of 90% Pmax (measured during the incremental test). An active rest of 6 min was used between these bouts, during which effort was per- formed with an intensity corresponding to the power achieved at VT1. During the first part of the experiment (1st–2nd week), all participants performed 4 bouts during HIIT. In the following weeks of the experiment (3rd–5th week), the participants performed 5 bouts during HIIT.
Low-intensity training (LIT) of 45–60 min, performed with intensity corresponding to the power achieved at Vt1. During the first part of the experiment (1st–2nd week), all participants performed 45 min of LIT. In the following weeks of the experiment (3rd–5th week), the participants performed 60 min of LIT.
Statistical analysis
Data were reported as mean, standard deviation, and confidence intervals. To assess the normality distribution of the data, the Shapiro-Wilk test was used. It was shown that the distribution of LOX-1 in the after-experiment measurements was statistically significantly different compared with the normal distribution in the POL, SIT and HIIT groups. In addition, the distribution of ox-LDL was different compared with the normal distribution in each group at before and after experiment measurements. With the other variables, no statistically significant differences were found compared to the normal distribution. Analysis of variance with repeated measures (ANOVA) was used to identify statistically significant main effects when the variables were not significantly different compared to a normal distribution. The Scheffe test was used as a post-hoc test. Where variables differed from a normal distribution, Friedman analysis of variance was used to compare differences between repeated measurements.
Before the experiment, the minimum study group size was estimated using the G-Power software, assuming a minimum very large 2 of 0.35 at p < 0.05 in the analysis of variance. In this way, it was determined that the entire study group should be at least 40 people. All statistical procedures were conducted using the Statistica 13 software.
Results
The ANOVA results revealed significant main effects for repeated measurements and mixed effects for repeated measurements and group concerning VO2max (F = 26.02, p = 0.000,η2 = 0.426 and F = 9.316, p = 0.000,η2 = 0.444, respectively), VO2max expressed in l min–1 (F =2 7.025, p = 0.000, η2 = 0.429 and F = 7.263, p = 0.000,η2 = 0.377, respectively), and Pmax (F = 48.133, p = 0.000, η2 = 0.572 and F = 8.615, p = 0.000,η2 = 0.418, respectively). Additionally, a significant effect of repeated measurements was observed for VEmax (F = 14.567, p = 0.001, η2 = 0.288). Post-hoc tests indicated that both VO2max and Pmax increased after the experiment in the POL and HIIT groups (Table 2).
Table 2
Physiological parameters measured before and after the experiment
POL – polarised training group, SIT – sprint interval training group, HIIT – high-intensity interval training group, LIT – low-intensity training group, VO2max – maximal oxygen uptake, Pmax – maximal aerobic power during the incremental test, Vemax – maximal pulmonary ventilation, RERmax – maximal exercise respiratory rate value, HRmax – maximal heart rate, mean – arithmetic mean value, CI – lower and upper confidence intervals
Using Friedman analysis of variance, statistically significant differences in repeated measurements for LOX-1 were demonstrated, when all study participants (n = 40) were included in the analysis without division into groups (χ2 = 5.158, p = 0.023), in the POL group (χ2 = 9.000, p = 0.003) and the HIIT group (χ2 = 4.500, p = 0.034) (Table 3). There were no statistically significant differences in repeated measurements for ox-LDL in any of the study groups (Table 3).
Table 3
LOX-1 and ox-LDL serum concentration before and after the experiment
POL – polarised training group, SIT – sprint interval training group, HIIT – high-intensity interval training group, LIT – low-intensity training group, LOX-1 – serum concentration of lectin-like oxidised low-density lipoprotein receptor-1, ox-LDL – serum concentration oxidised low-density lipoprotein, mean – arithmetic mean value, CI – lower and upper confidence intervals *
Discussion
The present study assessed the impact of four distinct training programs on maximal oxygen uptake, maximal aerobic power and cardiovascular health markers, such as serum LOX-1 and ox-LDL concentrations, in active individuals. The programs included: 1) a polarised training program incorporating SIT, long interval HIIT, and LIT; 2) a program focused solely on SIT; 3) a program focused solely on long interval HIIT; and 4) a program focused solely on LIT. It was shown that after 5 weeks of training in the POL group and HIIT group, the maximal oxygen uptake and maximal aerobic power increased and the LOX-1 concentration decreased. In turn, no statistically significant changes were observed in the SIT group and LIT group. In the POL group, Pmax and VO2max increased by 11.1% and 14.2%, respectively, and in the HIIT group by 10.2% and 9.5%, respectively.
The results of the presented study are similar to the study by Hebisz et al. [16], which compared the impact of two training programs on the aerobic capacity of cyclists. Hebisz et al. [16] showed that the POL program was more effective in improving aerobic capacity (VO2max and Pmax) than a program consisting of LIT and MIT. Both in the present study and the study Hebisz et al. [16] POL program incorporating SIT, long interval HIIT and LIT, the difference between the POL protocols was the number of training sessions, which were 5 training sessions per week for 8 weeks in the study by Hebisz et al. [16] and 3 training sessions per week for 5 weeks in the presented study.
The training programs applied in the POL and HIIT groups in the presented study showed high effectiveness compared to the studies by Helgerud et al. [26] and Astorino et al. [27], in which physically active individuals also performed at least 3 training sessions per week. Helgerud et al. [26] demonstrated that VO2max increased by 5.5% and 7.2% after 8 weeks of HIIT training performed by active individuals. Astorino et al. [27] obtained an increase in VO2max of 6% and 5.5% after 3 weeks of HIIT training performed by a group of men and women. Esfarjani and Laursen [28] showed that VO2max improved by 9.1% after 10 weeks of performing a training program incorporating HIIT and LIT.
Macpherson et al. [29] showed that after 6 weeks of running training, VO2max increased by 11.5% in a group performing SIT and by 12.5% in group performing LIT. An increase in VO2max by 12% was observed by Sökmen et al. [30] after 9–10 weeks of SIT training. Slightly smaller changes in VO2max (4–8%) were shown by Bailey et al. [31] and Zelt et al. [32] after 2–4 weeks of SIT training. In a meta-analysis, Vollaard et al. [33] showed consistent evidence that SIT increases VO2max. Other studies have shown that VO2max increased by 4–7% after 6–10 weeks of LIT training [30, 34]. In the presented study, no statistically significant changes in VO2max were observed in the SIT and LIT groups.
The duration of the SIT or LIT training program may affect the development of aerobic fitness, as no significant changes in VO2max were observed when the experiment lasted only two weeks [31, 35]. During longer duration experiments, 6–10 weeks, a significant improvement in aerobic capacity was observed [28–30]. Till et al. [36] suggest that the duration of the training intervention is important for achieving adaptive physiological changes. Perhaps in the presented study, 3 training sessions per week performed for 5 weeks among active individuals was too weak a training stimulus to improve aerobic capacity in the SIT and LIT groups. In the POL and HIIT groups, the duration and frequency of the training sessions were the same, but in these groups, the total time of high and/or maximal intensity efforts was greater than in the SIT and LIT groups. Moreover, Høydal [37] suggests that the effect of a training program on VO2max can be determined by the baseline level of aerobic capacity. In well-trained or physically active individuals with a high VO2max, it is more difficult to further improve the aerobic capacity in the training process, compared to individuals with a low VO2max and inactive individuals [37]. In the study Sökmen et al. [30], in which the greatest changes in aerobic capacity were obtained (VO2max increased by 12%), the groups performing a SIT and LIT training program had a baseline VO2max of approx. 40–42 ml · min–1 · kg–1. In the study by Zelt et al. [32], in which smaller changes in aerobic capacity were achieved (VO2max increased by 4%), the baseline VO2max was at 47–49 ml · min-1 · kg-1. In the presented study, the baseline VO2max levels in SIT and LIT groups were 47.6 ml · min-1 · kg-1 and 50.5 ml · min–1 · kg–1, respectively. Therefore, it seems conceivable that the replacement of the previous physical activity with SIT or LIT training with a total volume of approx. 3h per week was insufficient to significantly improve the aerobic capacity of the participants in the presented study.
In the presented study, no effect of the training programs used was observed on the changes of serum ox-LDL. Data in the available literature indicate that physical activity decreases ox-LDL levels in obese individuals [38]. Comparative data also indicate that levels of serum ox-LDL are lower in the athlete population (footballers) compared to physically inactive individuals [39]. However, according to tiainen et al. [20], the effects of training in reducing ox-LDL concentrations are dependent on the volume of training performed. tiainen et al. [20] observed a decrease ox-LDL concentrations in the group performing moderate- and high-intensity training sessions three or more times a week, and no change in ox-LDL in the group performing low- or moderate-intensity training less than three times a week. Therefore, it is possible that the three training sessions per week in the presented study were too weak a stimulus to reduce the serum ox-LDL concentrations.
Simultaneously, the results of the presented study showed that the POL and long interval HIIT programs were effective in reducing the serum LOX-1 concentrations, while no such effect was obtained after performing the SIT or LIT program. In the presented study, the expression of LOX-1 was not determined, only the concentration of its fragments dissolved in serum. Scientific research has analysed the expression and/or concentration of LOX-1 [40]. Assessing serum LOX-1 concentrations can be used to predict the risk of dangerous circulatory events, i.e., myocardial infarction or haemorrhagic stroke [41]. Hong et al. [19] suggested that strong shear stress associated with laminar flow occurs during exercise, which contributes to reduced LOX-1 expression. Shear stress is also thought to increase the release of platelet-derived microvesicles, which can stimulate angiogenesis [42]. The magnitude of the shear rate depends on the intensity of the exercises [42, 43]. Thijssen et al. [43] showed that the shear rate increases with the increasing exercise intensity. In the presented study, the POL and long interval HIIT programs were characterised by a higher total time of efforts performed at high intensity compared to the SIT and LIT programs. Referring to Thijssen et al. [43], it can be assumed that the shear stress stimulus may have exerted a stronger effect during the training performed by the POL and HIIT groups compared to the SIT and LIT groups. Perhaps, this allowed the POL and HIIT groups to experience changes in LOX-1 expression and thus a decrease in serum LOX-1 concentration [19].
Moreover, as reported by Gurd et al. [44] performing HIIT training affects increases in sirtuin 1 (SIRT1) activity and SIRT1 concentrations in skeletal muscle. It is believed that SIRT1 influences adaptation in skeletal muscle’s aerobic potential and may affect the regulation of LOX-1 activity [45]. Therefore, it is possible that the training programs used in the POL and long interval HIIT groups may have been effective in reducing the serum LOX-1 concentrations and in developing the VO2max and Pmax by affecting SIrt1 activity. In addition to changes in SIRT1 activity and concentrations, training programs containing HIIT efforts can decrease the activity of C-reactive protein and interleukins [46]. C-reactive protein and inter-leukin-18 affect the increased release of LOX-1 from macrophages into the blood [47]. Therefore, the POL and long interval HIIT programs may have influenced the reduction of serum LOX-1 concentrations through possible effects on lower pro-inflammatory protein activity.
Limitations
A limitation of the presented study is the participation of women in the training groups. The impact of women’s participation on study results was minimised by using block randomisation. Women were assigned evenly to each group because when divided into blocks, they were placed in the blocks with the lowest VO2max.
Another limitation of the presented study is that the oxidising factors, antioxidant factors, and inflammatory markers were not determined. Such markings could contribute to a better understanding of the results obtained. Therefore, further research is needed to determine changes in additional markers during the training process.
Conclusions
POL and long interval HIIT programs were effective in improving aerobic fitness in physically active individuals. Moreover, a reduction in serum LOX-1 concentrations was observed after completing the POL and long interval HIIT programs.
Practical application: for active individuals, we recommend choosing a polarised training program or a training program that includes long interval HIIT to improve cardiorespiratory fitness. POL and long interval HIIT programs are characterised by higher effectiveness in improving VO2max compared to programs that include SIT or LIT.