Introduction
Stress fractures are a significant clinical concern among female athletes, as they can affect both their overall health and their ability to train and compete effectively. Recurrent or improperly managed stress fractures may lead to reduced peak bone mass, increased susceptibility to future fractures, and long-term impairments in bone health and athletic performance, and in some cases even premature career termination [1]. These injuries result from repetitive submaximal loading on bone, outpacing the body’s capacity for remodelling and repair. They are present especially in endurance and weight-sensitive sports such as long-distance running, gymnastics, and ballet [2]. While intrinsic factors such as biomechanical alignment and bone geometry contribute to stress fracture risk, mounting evidence highlights a central role for low energy availability (LEA) and menstrual dysfunction – key components of both the Female Athlete Triad and the broader Relative Energy Deficiency in Sport (RED-S) model – in disrupting skeletal homeostasis [3].
LEA occurs when dietary energy intake is insufficient to support both training demands and essential physiological functions. This energy deficit impairs the hypothalamic–pituitary–gonadal (HPG) axis, leading to hypoestrogenism and menstrual irregularities such as oligomenorrhea and functional hypothalamic amenorrhoea [4]. Oestrogen plays a crucial role in bone formation and the inhibition of bone resorption. Its deficiency reduces bone mineral density (BMD) and contributes to microarchitectural fragility, increasing the susceptibility to stress-related skeletal injuries [5].
The Female Athlete Triad – comprising LEA, menstrual dysfunction, and low BMD – was the first clinical framework to link disordered energy balance with bone stress injuries in female athletes. The RED-S model expanded on this by recognising additional systemic effects of LEA, including impacts on immunity, cardiovascular health, and mental function, and by including male athletes [6]. Despite these advancements, underdiagnosis and delayed intervention remain prevalent, particularly among adolescent athletes, whose bone mass acquisition is not yet complete [7].
This review aims to explore the complex relationship between energy availability, menstrual health, and stress fractures in female athletes. It will discuss the current evidence regarding physiological mechanisms, diagnostic tools, risk stratification strategies, and evidence-based interventions. Recognising and addressing these interrelated factors is essential not only for injury prevention but also for preserving long-term skeletal and reproductive health in active females.
Stress fractures: pathophysiology and risk factors
Stress fractures are overuse injuries that result from the accumulation of repetitive submaximal forces on bone, exceeding its ability to remodel and adapt. The pathogenesis involves a disruption of normal bone remodelling – a dynamic process that balances osteoclastic resorption and osteoblastic formation in response to mechanical loading. In athletes, when the training intensity or frequency increases rapidly without adequate recovery or nutritional support, microdamage accumulates, leading to the development of a stress reaction and, ultimately, a fracture [8].
Female athletes are particularly vulnerable to stress fractures due to a combination of intrinsic and extrinsic factors. Anatomical and biomechanical differences, such as a wider pelvis and increased Q-angle, may contribute to altered lower extremity loading. However, physiological risk factors – especially those related to energy balance and hormonal health – are increasingly recognised as primary contributors [9].
Low energy availability (LEA), either from inadequate caloric intake or excessive energy expenditure, impairs multiple endocrine pathways critical to bone health. Most notably, LEA suppresses the HPG axis, leading to hypoestrogenism and subsequent menstrual dysfunction, both of which negatively affect bone mineral density.
In addition, LEA can affect the growth hormone, IGF-1 axis, leading to reduced insulin-like growth factor 1 (IGF-1) levels, which further limits bone formation and increases skeletal fragility [10]. Other hormone disruptions include elevations in cortisol and suppression of thyroid hormones, both of which also contribute to impaired bone turnover. Mechanistically, suppressed IGF-1 not only reduces osteoblast proliferation and collagen synthesis but also diminishes the anabolic response of bone to mechanical loading. Concurrently, elevated cortisol promotes osteoclast activity and downregulates osteoblast function, thereby shifting bone remodelling towards net resorption. Moreover, chronic cortisol elevation blunts growth hormone signalling, further aggravating IGF-1 suppression, creating a compounding effect that impairs bone regeneration and delays microdamage repair [11].
Extrinsic risk factors include training errors (e.g., sudden increases in mileage or intensity), poor footwear, hard training surfaces, and insufficient rest periods [12]. Athletes in sports emphasising leanness or aesthetics (e.g., distance running, gymnastics, figure skating) are at highest risk, due to both mechanical loading patterns and pressures to restrict energy intake.
Stress fractures in female athletes most commonly occur at high-load, weight-bearing sites, including the tibia, femur (neck and shaft), metatarsals, and pelvis. ‘High-risk’ stress fractures – such as those in the femoral neck, anterior tibial cortex, or navicular – are associated with delayed healing and higher complication rates, including complete fracture or nonunion [13]. Although stress fractures of the upper extremities and ribs are relatively uncommon compared to lower limb injuries, they do occur – particularly in athletes involved in repetitive, high-load upper body movements, such as gymnasts and tennis players. These injuries often develop insidiously and may go undiagnosed due to their nonspecific symptoms and the low clinical suspicion for stress-related pathology in these areas. Despite their rarity, these injuries can significantly impair performance and require prompt recognition and load modification for effective management and recovery [14].
Understanding the interplay of biomechanical loading, nutritional status, and endocrine function is essential for identifying at-risk athletes and implementing targeted prevention strategies. As evidence accumulates, it is increasingly clear that maintaining adequate energy availability and menstrual regularity is fundamental to preserving bone integrity and athletic longevity in women.
Prevalence of stress fractures in female athletes: a sex-based comparison
Stress fractures are among the most common overuse injuries in athletic populations, with a disproportionately higher incidence in female athletes compared to their male counterparts. Epidemiological studies suggest that female athletes are 1.5 to 3 times more likely to develop stress fractures than males, particularly in endurance and aesthetic sports such as distance running, gymnastics, figure skating, and dance. A large prospective study of collegiate athletes found that female athletes with multiple components of the Female Athlete Triad had a significantly increased risk of bone stress injuries [15]. Specifically, the incidence of stress fractures increased from 15% in low-risk athletes to 30% in those classified as high-risk based on Triad-related factors (e.g., menstrual dysfunction, low energy availability, and low bone mineral density).
By contrast, male athletes tend to have lower rates of energy deficiency and hormone disruption, which may explain their comparatively reduced risk for stress fractures. However, RED-S is increasingly recognised in males, especially in weight-sensitive and endurance sports (e.g., cycling, rowing, and distance running), where disordered eating behaviours and chronic under-fuelling can occur. It is also worth noting that research shows that military training significantly increases the prevalence of stress fractures in men, with reported incidence rates as high as 8% primarily due to high-impact, repetitive loading activities such as marching, running, and jumping under load.
The site of injury also differs between the sexes. In women, stress fractures are more frequently observed in the pelvis, femoral neck, and tibia, while men more commonly experience fractures in the metatarsals, tibia, and fibula. This discrepancy may reflect sex differences in biomechanics, bone geometry, and hormonal influences, particularly oestrogen’s protective role in female skeletal health [16].
Although RED-S now provides a unified framework for both sexes, current literature and screening tools are still more extensively validated in female athletes. More data are needed to clarify sex-specific thresholds for energy availability, hormone dysfunction, and fracture risk in men, as highlighted in Table 1. However, the screening tools available now are largely based on female data and lack the diagnostic cutoffs specific to men, limiting accurate risk assessment in male athletes.
Table 1
Comparison of sex-specific patterns in stress fracture risk and related endocrine factors in athletes
Ultimately, while stress fractures affect both sexes, the prevalence is consistently higher in female athletes, largely due to the greater incidence of LEA, menstrual dysfunction, and compromised bone health. A sex-specific approach to screening, prevention, and education is critical to reducing the burden of these injuries in both athletic populations.
Energy availability in athletes
Energy availability (EA) refers to the dietary energy remaining after exercise, normalised to fat-free mass (FFM). An EA below 30 kcal/kg FFM/day is defined as LEA and is insufficient to support essential physiological processes. LEA, whether intentional or unintentional, is prevalent in female athletes – particularly in endurance and aesthetic sports – and is a primary driver of hormone disruption and impaired bone health [17].
LEA suppresses the hypothalamic–pituitary–gonadal axis, leading to reduced oestrogen and functional hypothalamic amenorrhoea (FHA), both of which are associated with decreased BMD and increased stress fracture risk. Other hormonal effects include reduced IGF-1, triiodothyronine (T3) and leptin, and elevated cortisol, further impairing bone remodelling [18].
Due to difficulties in directly measuring EA, screening tools such as the Low Energy Availability in Females Questionnaire (LEAF-Q) and RED-S Clinical Assessment Tool (RED-S CAT) are useful for identifying at-risk athletes based on menstrual, gastrointestinal, and injury symptoms. Even short-term LEA can alter bone turnover markers, and in adolescents, it can compromise peak bone mass development [19]. Recognising LEA early is critical for preventing bone injury and preserving long-term athlete health.
Menstrual dysfunction and bone health
Menstrual dysfunction is a well-recognised consequence of LEA and a critical mediator of bone loss in female athletes. The spectrum includes luteal phase defects, oligomenorrhea (menstrual cycles > 35 days), and FHA, all of which are associated with reduced oestrogen levels and impaired bone health.
Oestrogen plays a vital role in maintaining bone integrity by inhibiting osteoclast-mediated bone resorption and promoting osteoblast activity. In hypoestrogenic states – common in athletes with FHA – there is an increase in bone turnover and a net loss of bone mass, particularly at trabecular-rich sites such as the lumbar spine and pelvis. Adolescent and young adult athletes are especially vulnerable, as they may fail to achieve peak bone mass, leading to long-term skeletal fragility.
Longitudinal data indicate that even subclinical menstrual disturbances (e.g., subtle luteal phase defects) can negatively impact bone accrual and increase the risk of stress fractures. Moreover, the duration of amenorrhoea is directly correlated with the degree of BMD loss and fracture risk, highlighting the importance of early detection and intervention.
Bone loss in amenorrheic athletes is often partially reversible with restoration of energy availability and resumption of regular menses. However, complete recovery of BMD may not always occur, particularly if the condition develops during adolescence or persists for extended periods. Pharmacological interventions such as oral contraceptives (OCPs) have been used, but current evidence suggests they may mask the problem without restoring endogenous oestrogen production or improving bone density [20].
Importantly, menstrual dysfunction is not always reported by athletes and is frequently normalised in sport culture. Coaches and healthcare providers must proactively inquire about menstrual regularity and educate athletes that irregular or absent menses are not benign signs of ‘fitness’, but rather markers of under-fuelling and compromised health.
The Female Athlete Triad vs. RED-S
The Female Athlete Triad and RED-S are two interrelated clinical frameworks developed to describe the adverse physiological effects of LEA in athletes. Although they share similar foundations, they differ in scope and diagnostic application.
The Female Athlete Triad, first defined in the 1990s, comprises three interrelated components: low energy availability (with or without disordered eating), menstrual dysfunction, and BMD.
The triad was originally conceptualised to describe health concerns in female athletes, particularly those participating in sports that emphasise leanness, aesthetics, or endurance. It laid the foundation for identifying key risk factors for stress fractures, including functional hypothalamic amenorrhoea and reduced BMD [20].
Recognising that LEA affects multiple organ systems beyond reproduction and bone, and that male athletes can also be affected, the International Olympic Committee (IOC) introduced the RED-S model in 2014, with an updated consensus in 2018. RED-S includes a wider array of potential consequences of LEA, affecting metabolic rate, menstrual function, bone health, immunity, protein synthesis, cardiovascular and gastrointestinal function, and psychological well-being.
The RED-S model also emphasises the performance consequences of LEA, such as increased injury risk, impaired judgement, decreased coordination, and reduced endurance. Its diagnostic and monitoring tools, including the RED-S CAT, enable clinicians to stratify risk and guide return-to-play decisions.
While RED-S is broader, the Female Athlete Triad remains clinically useful, particularly in female populations where menstrual dysfunction and bone loss are evident. Triad-specific tools, such as the triad cumulative risk assessment score, provide targeted guidance for managing and monitoring at-risk athletes. Some clinicians use the triad as a subset within RED-S, focusing on its measurable reproductive and skeletal components [21].
Despite these advances, both models face challenges in clinical use, including underreporting of menstrual dysfunction, difficulty in measuring energy availability directly, cultural normalisation of under-fuelling in sport, and limited awareness among coaches and nonspecialist providers. Combining both models allows for a comprehensive and individualised approach.
Diagnosis and monitoring
Early and accurate identification of athletes at risk for stress fractures is essential for effective prevention and intervention. However, diagnosis is often delayed or missed due to the underreporting of symptoms, normalisation of menstrual irregularities in sports culture, and the absence of a single diagnostic test for LEA. Additionally, clinicians should consider important differential diagnoses when evaluating athletes with similar presentations, including medial tibial stress syndrome (MTSS), osteomyelitis, bone tumours, and inflamma-tory or metabolic bone conditions, which may mimic early stress injuries.
Comprehensive clinical assessment
A thorough clinical history remains the cornerstone of diagnosis. Key areas of inquiry include menstrual patterns (age at menarche, cycle regularity, history of amenorrhoea), energy intake, dietary habits, and intentional or unintentional caloric restriction, training load and recent changes in exercise volume or intensity, history of previous fractures or injuries, gastrointestinal symptoms, fatigue, and mood changes and body image concerns or disordered eating behaviours.
Physical examination may reveal signs of undernutrition, including low BMI, bradycardia, orthostatic hypotension, dry skin, or hair loss, though many athletes may appear outwardly healthy [22].
Screening tools
Several validated screening tools support clinical assessment: LEAF-Q: A self-report tool that assesses menstrual history, gastrointestinal function, and injury frequency. A score 8 suggests a high risk for LEA.
RED-S CAT: Provides a colour-coded risk stratification system (green, yellow, red) to guide medical clearance and return-to-play decisions.
Triad cumulative risk assessment (TCRA): Used to classify athletes into low-, moderate-, or high-risk based on menstrual, energy, and BMD status [23].
Laboratory investigations
Laboratory tests can support clinical diagnosis and help rule out other causes of menstrual irregularity or bone loss. Recommendations include: reproductive hormones: LH, FSH, estradiol (often suppressed in functional hypothalamic amenorrhoea); thyroid function: thyroid-stimulating hormone (TSH), free thyroxine (T4); cortisol: elevated in chronic stress or energy deficiency; prolactin: elevated levels may indicate other causes of amenorrhoea; 25(OH) vitamin D and calcium: to assess bone health; IGF-1: a marker of energy availability and anabolic activity [24].
Imaging and bone density evaluation
Dual-energy X-ray absorptiometry (DXA) is the gold standard for assessing BMD. Particular attention should be given to the lumbar spine, femoral neck, and total body. In adolescent athletes, BMD Z-scores below –1.0 warrant concern, while a Z-score –2.0 is consistent with low bone mass for age [24].
MRI is the preferred modality for diagnosing stress fractures, especially early-stage stress reactions or subtle bone marrow oedema not visible on X-ray [25].
Regular monitoring
Moderate-to- high-risk athletes should undergo regular monitoring, including menstrual tracking, cautious evaluation of weight and body composition, DXA scans every 12–24 months, and psychological assessment when needed. A multidisciplinary team approach is essential, and education is critical, as many athletes overlook symptoms like menstrual changes or fatigue as signs of underlying health issues [26]. Key imaging and monitoring strategies are summarised in Table 2.
Table 2
Imaging and monitoring in athletes at risk of stress fractures
Management and prevention
Preventing stress fractures in female athletes requires addressing the root cause through a comprehensive, multidisciplinary approach focused on early identification, behavioural change, nutritional support, and, when necessary, medical or psychological intervention.
The primary goal of treatment is to restore energy availability by increasing caloric intake, reducing energy expenditure, or both. This often requires collaboration with a sports dietitian to ensure athletes are meeting their energy, macronutrient, and micronutrient needs, including: calcium ( 1,500 mg/day) and vitamin D ( 800–1,000 IU/day) to support bone remodelling and reduce fracture risk, and adequate protein intake ( 1.6 g/kg/day) to support bone and muscle health [27].
Correcting LEA often leads to the resumption of menstrual function, which is an important marker of physiological recovery. However, in some cases, especially when amenorrhoea is prolonged or psychological barriers persist, additional treatment strategies may be required [28].
Athletes may need to temporarily reduce training volume or intensity to allow for bone healing and physiological recovery. Cross-training with low-impact activities (e.g., swimming or cycling) can help maintain cardiovascular fitness while minimising skeletal stress.
The role of hormone therapy in treating amenorrheic athletes remains debated. Combined oral contraceptives (COCs) have traditionally been prescribed to ‘regulate’ menstruation, but evidence suggests they do not improve bone mineral density in the context of LEA or functional hypothalamic amenorrhoea. Instead, transdermal oestrogen with cyclic progesterone may be more effective for improving BMD in adolescents and young adults with FHA.
Hormone therapy should not replace nutritional rehabilitation, which is essential for restoring energy balance and normal hormone function. However, in cases of persistent amenorrhoea or low bone mineral density despite adequate nutrition, hormone treatment – preferably transdermal oestrogen with cyclic progesterone – may be considered under the care of an endocrinolo-gist. It should be used as a supportive measure, not a primary solution [29].
Many athletes with LEA or disordered eating behaviours benefit from mental health support, particularly if there is body image distortion, anxiety around weight gain, or performance pressures. Cognitive-behavioural therapy (CBT) is commonly used to address maladaptive thought patterns and support behaviour change [30].
Prevention begins with the early education of athletes, coaches, and families. Creating a supportive team culture that values health over appearance is critical for the long-term prevention of LEA and its consequences.
Return to sport and long-term considerations
The decision to return an athlete to full sport participation after a stress fracture requires a cautious, individualised approach. The goal is to ensure both bone healing and physiological recovery, while also addressing any underlying behavioural, nutritional, or psychological contributors to the injury.
Criteria for return to play
Return-to-play (RTP) decisions should be guided by a multidisciplinary team [31] and based on clinical healing: resolution of pain and full, ache-free function during activity; and radiographic confirmation: evidence of bone healing on imaging, especially for high-risk fracture sites such as the femoral neck or navicular bone.
Other clinical factors include resumed menstrual function (if previously absent) or demonstrable progress towards hormone normalisation; and correction of LEA: restoration of adequate energy intake and stable weight. Another crucial factor is psychological readiness: absence of anxiety or disordered eating behaviours that may compromise recovery.
The RED-S CAT can support stratifying risk and guiding RTP progression. Athletes in the ‘red zone’ (e.g., with severe LEA, active eating disorders, or recurrent fractures) should be withheld from training and competition until stabilised [31].
Return-to-activity progression
A graduated return-to-sport plan is recommended, beginning with an initial phase of non-weight-bearing or low-impact activities such as swimming or cycling. This is followed by the reintroduction of weight-bearing through light loading and a gradual increase in intensity. Once tolerated, the athlete can progress to sport-specific training with a controlled return to full activities. Full competition is only advised once the athlete is asymptomatic and bone health, along with energy availability, has been normalised, as pictured in Figure 1.
Figure 1
Return-to-sport protocol after stress fracture, progressing from low-impact activity to gradual loading, sport-specific training, and full return to competition
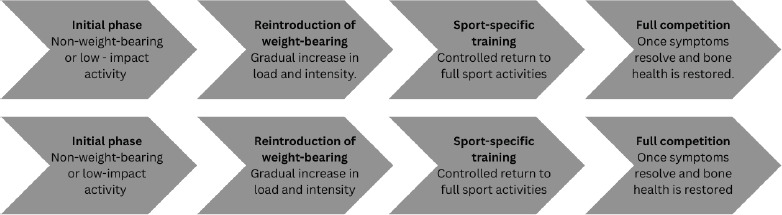
This process may take 8–16 weeks or longer, depending on injury location, severity, and individual recovery.
Long-term management includes menstrual tracking, periodic BMD assessment via DXA (every 12–24 months), monitoring of nutritional status and energy balance, and ongoing mental health support – especially in athletes with prior low BMD, stress fractures, or disordered eating [32].
Athletes who develop stress fractures during adolescence – when peak bone mass is still being accrued – may be at long-term risk of reduced bone strength, even if menstruation resumes. Ensuring optimal bone health during these critical years is essential for preventing premature osteopenia or osteoporosis later in life.
Future directions and research gaps
Despite the growing awareness of the role of LEA and menstrual dysfunction in stress fractures among female athletes, important gaps remain in our understanding, detection, and management of these interrelated conditions.
While tools such as the LEAF-Q and RED-S CAT have improved clinical screening, they rely heavily on self-reported symptoms, which are often under-recognised or under-reported by athletes. There is a pressing need to develop and validate objective biomarkers of LEA – such as IGF-1, leptin, or bone turnover markers – that could allow earlier identification of at-risk individuals before clinical consequences arise [33].
Adolescence is a critical period for bone mass accrual, yet limited long-term data exist on whether athletes who develop stress fractures during this stage regain normal BMD and fracture resistance later in life. More longitudinal cohort studies are needed to track recovery trajectories and evaluate the irreversibility of bone loss associated with prolonged amenorrhoea or chronic LEA [34, 35].
The effectiveness of hormone therapies also warrants further investigation. Emerging research suggests that transdermal oestrogen with cyclic progesterone may improve BMD in hypoestrogenic females, but further randomised controlled trials are needed to confirm optimal hormone regimens, treatment timing, and their long-term safety and efficacy in young athletes [36, 37]. The potential role of vitamin D in supporting bone health in this population also deserves further exploration [38].
Furthermore, there is currently no standardised screening protocol for the early detection of LEA-related bone stress in sports settings. Existing tools are not fully validated across different sports, age groups, or in male athletes, and there is no consensus on screening frequency or biomarker thresholds. This variability often results in delayed recognition, inconsistent monitoring practices, and a predominantly reactive rather than preventive clinical approach, limiting opportunities for early intervention and multidisciplinary management.
Conclusions
Stress fractures in female athletes are multifactorial injuries with strong links to LEA, menstrual dysfunction, and impaired bone health. These interrelated conditions, outlined in both the Female Athlete Triad and the broader RED-S framework, have substantial implications not only for skeletal integrity but also for long-term reproductive, metabolic, and psychological health.
Effective prevention and management require early identification, targeted nutritional and behavioural interventions, and a multidisciplinary care model. Tools like the LEAF-Q, RED-S CAT, and bone mineral density assessments can aid in diagnosis and monitoring, but further refinement of objective biomarkers and risk stratification methods is needed.
Despite consensus statements and guidelines, awareness of LEA and RED-S remains low among athletes, coaches, and even healthcare providers. Research should continue to assess the impact of educational interventions at the team, institutional, and community levels, and how early prevention programs can be integrated into both youth and elite sport settings.
Future research should also address longitudinal outcomes, particularly in adolescents, and evaluate the safety and efficacy of hormone therapies in restoring bone mass and normal endocrine function. Bridging these knowledge gaps will be critical in protecting both performance capacity and lifelong health in female athletes.
Ultimately, a cultural shift that prioritises health over appearance or leanness is essential. Promoting energy balance, menstrual health, and skeletal resilience should be foundational to training environments that foster sustainable athletic success.