Introduction
Among the various strength enhancement methods, isometric training is an effective athletic performance improvement strategy [1]. Its primary characteristic is the absence of external movement during contraction [2]. In addition, owing to its risk-benefit ratio, it represents an attractive alternative to dynamic training [3]. Research on factors influencing strength development in isometric training, such as contraction duration [4], contraction speed [5], tendon characteristics [3], and muscle length [6], is available in the literature. However, most publications focus on the effects of isometric training on the lower body. Regarding the upper body, isometric contractions have mainly been used in reha bilitation, including shoulder stabiliser muscle coactivation assessment [7] and neck-shoulder pain treatment [8].
Few studies have focused on isometric training at short muscle lengths [9, 10], in which neural adaptations are primarily responsible for strength gain [6]. Constant feedback from the neuromuscular spindles is essential for muscle contraction positions at short joint angles and requires gamma motor neurons to stretch the intrafusal fibres; otherwise, a communication deficit between the muscle and central nervous system would occur [11]. Moreover, Carolan and Cafarelli [12] demonstrated that strength improvements in isometric training depend on antagonist co-contraction reductions. Thus, maintaining constant muscle-nervous system communication is essential to complying with the law of reciprocal inhibition and regulating this antagonist co-contraction [11]. this factor is even more necessary in joints, such as the shoulder, which is the most mobile in the human body and requires effective muscle stabilisation [7].
Although various types of muscle training have been investigated, few studies have compared isometric and high-speed dynamic contractions. these contractions, known as dynamic or ballistic stretching (BS), have been used historically in sports warm-ups as they can simulate the competition movements. they are characterised by fast movements in which the mass is accelerated to the end of the range of joint mobility [13], in other words, maximal muscle shortening. In throwing sports, ballistic shoulder movements are the key technical elements of competition [14]. As such, one and two-handed throws are used in performance evaluation and are considered simple, reliable, and close to the sporting gesture [15]. Nonetheless, studies on the acute effects of BS on sporting performance have yielded favourable [13], non-significant [16], and negative effects [17].
Despite investigations on the effects of isometric contractions on different muscle lengths [10], they have yet to be studied in maximally shortened positions. Furthermore, there are few studies on the effects of BS on the shoulder compared to those on the lower body [13], despite the number of sports in which upper-body performance is critical. Similarly, isometric training has not been compared with protocols involving BS. therefore, this study compared the acute effects of BS and voluntary isometric contractions at maximal shortening (VICAMS) as part of a warm-up on strength, range of motion, and release. We hypothesised that VICAMS would augment active range of motion (Arom), maximal voluntary isometric force (MVIF), and one-handed [unilateral seated shot-put test (USSPT)] and two-handed [seated shot-put test (SSPT)] throw lengths than BS.
Material and methods
Participants
Sixty healthy recreationally active subjects [30 females and 30 males; age = 46.4 ± 5.5; height = 1.70 ±0.17 m; weight = 76.0 ± 14.9 kg; body mass index (BMI) = 25.5 ± 2.5 kg/m2] voluntarily enrolled in this study. the eligibility criteria were age between 35 and 55 years and engaging in non-competitive physical activity at least twice a week. Exclusion criteria were shoulder injuries, such as rotator cuff tears, adhesive capsulitis, or scapulothoracic fusion, which prevented correct test performance and reduced measurement reliability [18].
Individuals engaging in recreational physical activity at various sports centres were invited to participate, with the first 30 men and 30 women meeting the established criteria selected. the recruitment process took place over two months prior to the start of testing. the participants were unfamiliar with the tests performed and were informed that they should not engage in physical activity the day before the test. during the familiarisation sessions, the study design was explained to the athletes, and they were allowed to ask questions.
Design and procedures
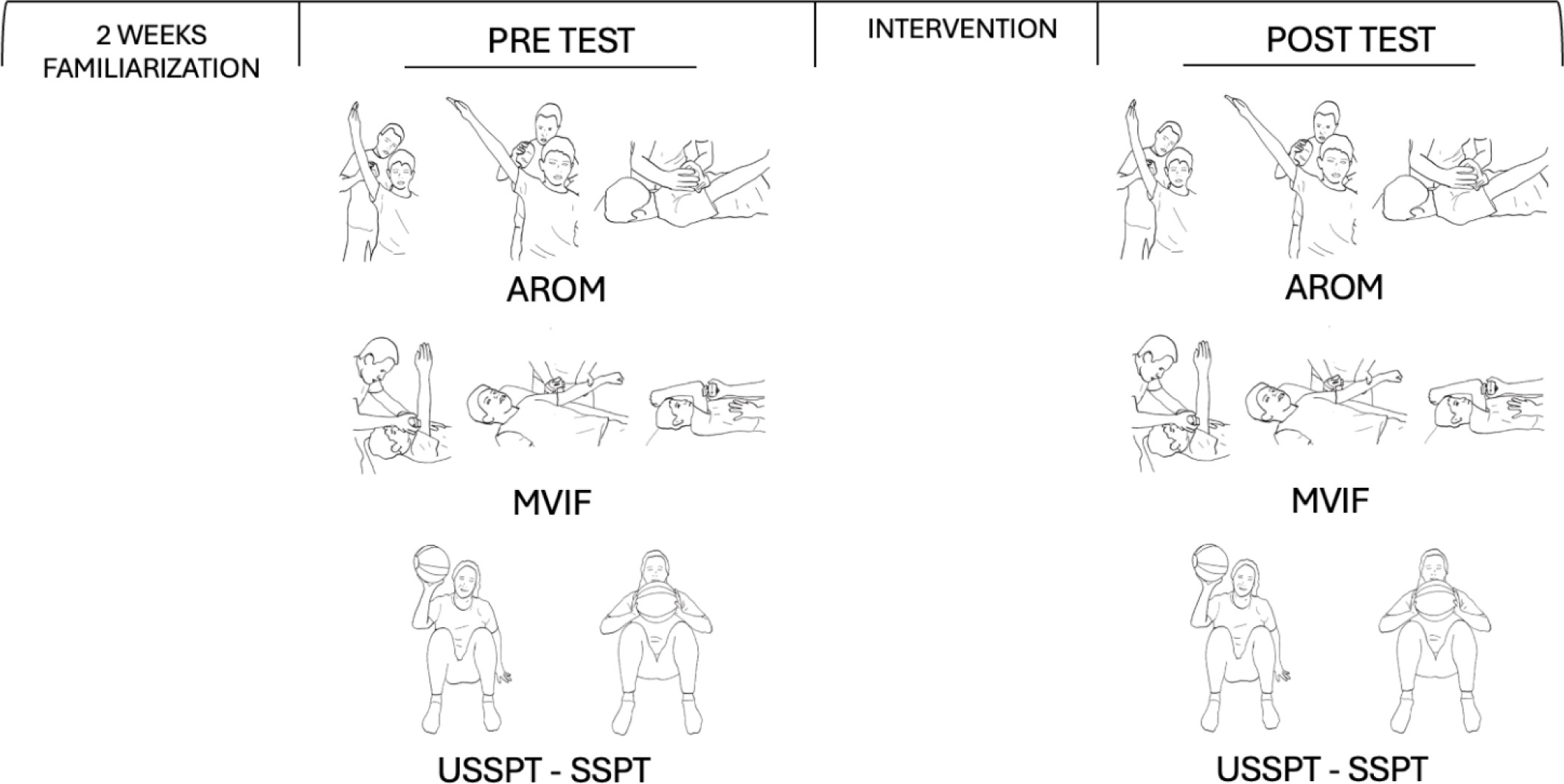
A randomised controlled repeated-measures design was used to assess and compare the acute effects of VICAMS and BS on AROM, MVIF, USSPT, and SSPT. Participants underwent two weeks of test familiarisation and various exercises before starting the measurements. They were then randomly assigned to a VICAMS group (n = 20), BS group (n = 20), or control group (CG) (n = 20), with males and females equally distributed between each. AROM, MVIF, SSPT, and USSPT were used to assess acute effects before and after the intervention. The AROM and MVIF measurements were performed in shoulder flexion (SF) and shoulder extension (SE). The CG did not undergo any intervention and was measured again 20 min after the first measurement.
Before starting, the participants were required to complete a standardised shoulder warm-up consisting of 10 flexion-extensions, 10 abductions, 10 external rotations, 10 internal rotations, and 10 horizontal abduction-adductions. They performed the first half with slow movements and the other half in a ballistic manner and were instructed to reach the maximum possible joint shortening in each repetition. Finally, three two-arm throws with a 5 kg medicine ball and three throws with each arm with a 3 kg medicine ball were performed. The warm-up was followed by a 10-minute rest period before the first measurement to minimise its effect. The measurements were then taken in the following order: (1) AROM (3-minute pause); (2) MVIF (3-minute pause); (3) SSPT (3-minute pause); (4) USSPT (5-minute pause); (5) Intervention (5-minute pause); (6) AROM (3-minute pause); (7) MVIF (3-minute pause); (8) SSPT (3-minute pause); (9) USSPT. A schematic representation of the study design is shown in Figure 1. All measurements were taken by the principal investigator, who has a degree in sports science and extensive experience in this area. the study took place at the BioReed Lab, Puerto de la Cruz, Tenerife (Spain), which was maintained at approximately 23°C.
Measures
Active range of motion measures
AROM measurements of the glenohumeral joint were performed according to the method described by Clarkson [19]. A calibrated hand-held digital goniometer-dynamometer (Micro-FET3; Hoggan Scientific, Ur, USA), which provides reliability and ease of use, measured AROM and MVIF [20]. SF was measured first with the participant seated, the back upright, and the arm at the side with the palm directed medially. For the initial measurement, the goniometer was placed on the anterior side of the arm, just above the elbow. The participant slowly moved the extended arm forward and upward until reaching the limit of movement, where the final measurement was taken. He/she then returned to the initial position, with the process repeated three times. Subsequently, the SE was measured in the prone position, with the arm at the side and the palm facing medially. The goniometer was placed on the back of the arm, just above the elbow, to take the initial measurement. The participant slowly moved the extended arm upwards until reaching the limit of movement, where the final measurement was taken. The participant then returned to the starting position, and the process was repeated three times. The largest measurements were used for further analysis. The investigator ensured that the scapula was fixed so no compensatory movements occurred. A 10-second rest was taken between measurements to minimise the effect of fatigue, with 30 s between positions to anchor the participant’s posture.
Maximal voluntary isometric force measures
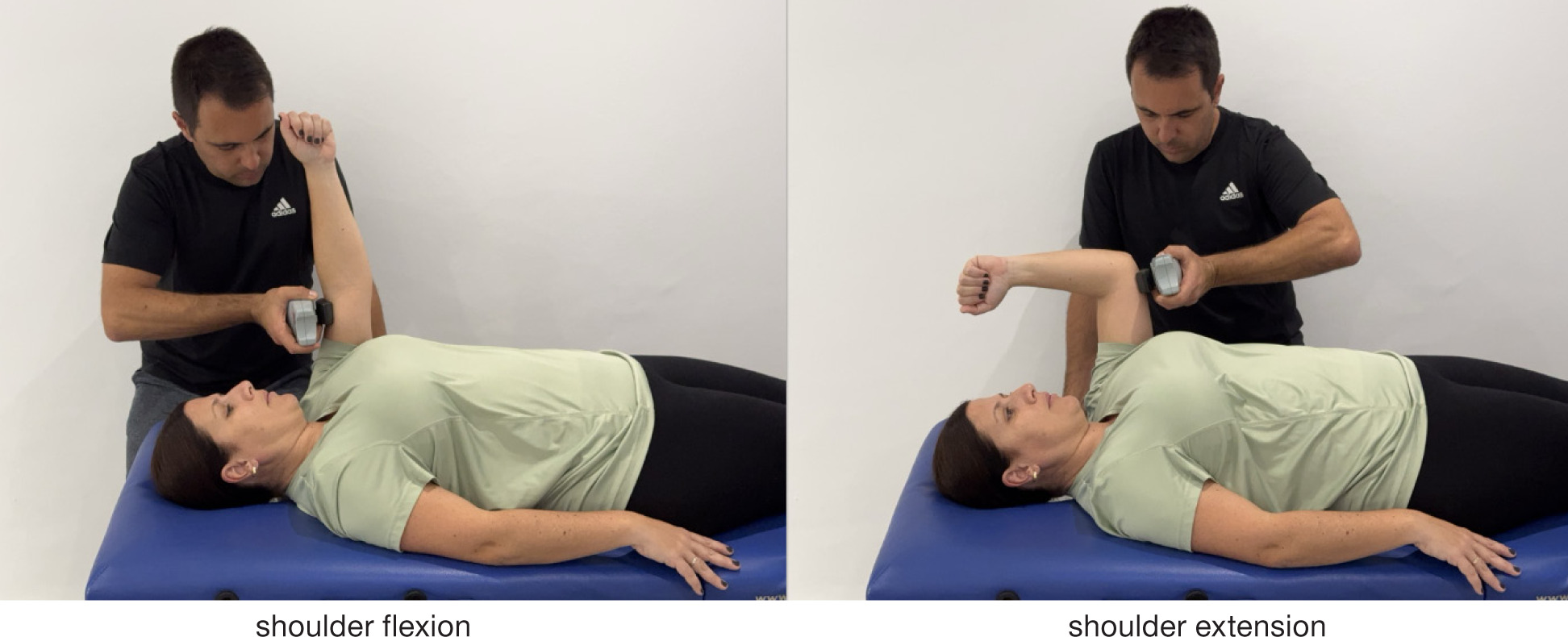
All measurements used the positions and techniques described by Andrews [21]. Force measurements were expressed in Newtons, and values were provided by our scientifically validated device (Microfet 3; Hoggan Scientific, UT, USA). To measure the SF, the participant was supine with the shoulder flexed 90°, the elbow extended, and the palm facing medially. The dynamometer was placed on the front of the upper arm just proximal to the epicondyle of the humerus. To measure SE, the participant was supine with the shoulder flexed 90°, the elbow flexed, and the palm facing medially. The dynamometer was placed on the back of the upper arm just proximal to the epicondyle of the humerus. The positions used are shown in Figure 2. As in the previous protocol, the SF was measured first, then theSE, with three measurements taken and the largest used for analysis [22]. For its execution, participants were instructed to exert as much force as possible against the device while the researcher held the device as still as possible without breaking the position. this methodology, known as a make test, is used almost exclusively with hand-held dynamometry [23]. the subjects rested for 15 s between measurements and 30 s between positions to minimise the effect of fatigue. Participants gradually increased to maximal strength and maintained the effort for 5 s, which was sufficient to reach maximal strength [24].
Seated shot-put test measures
Three 5 kg medicine ball throws were performed [15, 25], with 30 s of rest between each attempt, and the best mark was used for the analysis. the distance from the chest to the point of impact with the ground was measured using a tape measure and expressed in metres. these methods have excellent reliability and provide a practical and effective measure of upper-limb functional power [15, 25]. during the warm-up, the participants practised the throwing technique and adjusted their angle to throw the ball as far as possible, simulating a movement similar to the chest pass in basketball [25]. For the measurement, the subject sat on the floor with their back against a wall with their knees flexed at approximately a right angle, and their feet applied force backwards to maintain a firm position against the wall [26]. they held the ball with both hands up to their chest and threw it as far as possible, following the technique practised during the warm-up. the ball was coated with magnesium powder to prevent slipping and ensure a strong, reliable grip. the closest mark on the ground was used to measure the throw accurately. Only throws that were correctly executed within the lane were considered. the throw test was repeated for any mismatch that could affect the measurement after a consistent recovery time. Verbal encouragement was provided to promote maximum effort in the throw [15].
Unilateral seated shot-put test measures
The USSPT measurements were similar to the SSPT measurements, except for the ball weighing 3 kg and the throwing technique. In this case, the participants were instructed to position their arms like an athletic weight thrower before executing the throw. the back was supported on a 33 cm column that allowed freedom of movement of the throwing arm.
Interventions
Ballistic stretching intervention
The exercises were performed with each arm in the following order:
SF: the participant was standing with arms extended towards the floor and palms facing the body and was instructed to raise one arm forward with the elbow extended and return to the starting position.
SE: the participant was standing with arms extended towards the ground and palms facing the body and was instructed to raise one arm behind with the elbow extended and return to the starting position.
Shoulder abduction (SABD): the participant was standing with arms extended towards the ground and palms facing forward and was instructed to raise one arm to the side with the elbow extended as close to the head as possible and return to the starting position
Shoulder internal rotation (Sir): the participant was supine on the side of a stretcher with one arm outside the stretcher. To reach the starting position, the participant performed a 90° elbow flexion, 90° shoulder abduction, and maximum shoulder external rotation. the exercise consisted of bringing the hand to maximum internal rotation and returning to the initial position, keeping the elbow in flexion and the shoulder in abduction.
External shoulder rotation (SER): the participant was prone on the side of a stretcher with an arm hanging towards the floor. the participant performed a 90° horizontal shoulder abduction and 90° elbow flexion to reach the starting position. the exercise consisted of bringing the hand to the ceiling in front and returning to the starting position, keeping the elbow in flexion and the shoulder in abduction.
Three sets of 20 s were performed with each arm and exercise, recovering for 10 s after each set. the intervention lasted approximately 15 min. A rhythm of 40 beats per minute (bpm) was established and controlled using a metronome. the subject’s arm returned to the starting position for each repetition of the full range of motion. the subject was instructed to perform the movement following the metronome rhythm and reach the maximum possible joint shortening in each repetition.
Voluntary isometric contraction at maximal shortening intervention
The exercises were performed as follows:
SF: In the supine position, force was applied just above the elbow in the direction of SE while keeping the elbow extended.
SA: In the supine position, force was applied just above the elbow in the direction of shoulder adduction while keeping the elbow extended.
SIR: In the supine position, with the shoulder abducted to 90° and the elbow flexed to 90°, force was applied to the wrist in the direction of the shoulder external rotation (SER). the scapula was stabilised to prevent compensatory movements.
SER: In the supine position, with the shoulder abducted to 90° and the elbow flexed to 90°, force was applied to the wrist in the direction of the SIR. the scapula was stabilised to prevent compensatory movements.
SE: In the prone position, force was applied just above the elbow in the direction of SF while keeping the elbow extended.
For the execution of each exercise, the joint was brought to maximum muscle shortening and force was applied in the opposite direction of the movement. the participants were instructed to perform a push contraction to resist this force without overcoming it. After each repetition, the position of maximum joint shortening was maintained without returning to the initial position. three actions were performed before each exercise to optimise muscle contraction, including showing the approximate location of the main muscles to be exercised, palpating several points of these muscles with the fingers, and asking the participant for maximum concentration. the forearm was kept perpendicular to the segment where the force was applied to avoid the involvement of other muscles. the execution of each exercise was verbally guided by instructions to contract, hold, and relax. Nine repetitions (5 s each) of each movement were performed, applying force at different intensities, including light (20-30%), medium (45-55%), and maximum (100%). Individual intensity thresholds were recorded for each subject to work in their zone. Rests of 3 s were recorded between repetitions, 15 s between each arm, and 30 s between exercises. the duration of the intervention was similar to that of the previous protocol.
Statistical analysis
Standard statistical methods were used to calculate the mean and standard deviation (SD). the Kol- mogorov-Smirnov test confirmed that the data had a normal distribution. the sample size was calculated using GRANMO version 7.12 (Barcelona, Spain), with a 5% significance level and 80% statistical power, indicating that 14 participants were required for each group. Based on previous studies [27], the standard deviation was 6.4°. Student’s independent samples t- test compared the baseline characteristics of the participants. Since there were no between-group differences at baseline, a two-way (group x time) repeated-measures analysis of variance (ANOVA) with Bonferroni’s post hoc evaluated group-by-time interactions and with- in-group and between-group effects. A confidence interval (CI) of 95% was obtained for all differences, and effect size (ES) was obtained for significant differences. ES was interpreted as small (0.1), moderate (0.3), large (0.5), very large (0.7), or extremely large (0.9) using Cohen’s d [28]. All analyses employed SPSS version 21.0 (IBM Corp., NY, USA), with statistical significance set at p < 0.05.
Results
Tables 1 and 2 show all data regarding Arom, MVIF, SSPT, and USSPT variables of all participants, according to their group. Main time effects and time*group interactions were found for all variables (p < 0.001).
Table 1
Mean and standard deviation data for active range of motion, maximal isometric strength (shoulder), seated shot-put test, and unilateral seated shot-put test. Pre and post-measurements for participants in all groups are also shown
Table 2
Intra-group and between-group differences for active range of motion, maximal isometric strength (shoulder), seated shot-put test, and unilateral seated shot-put test. Pre and post-measurements for participants in all groups are also shown
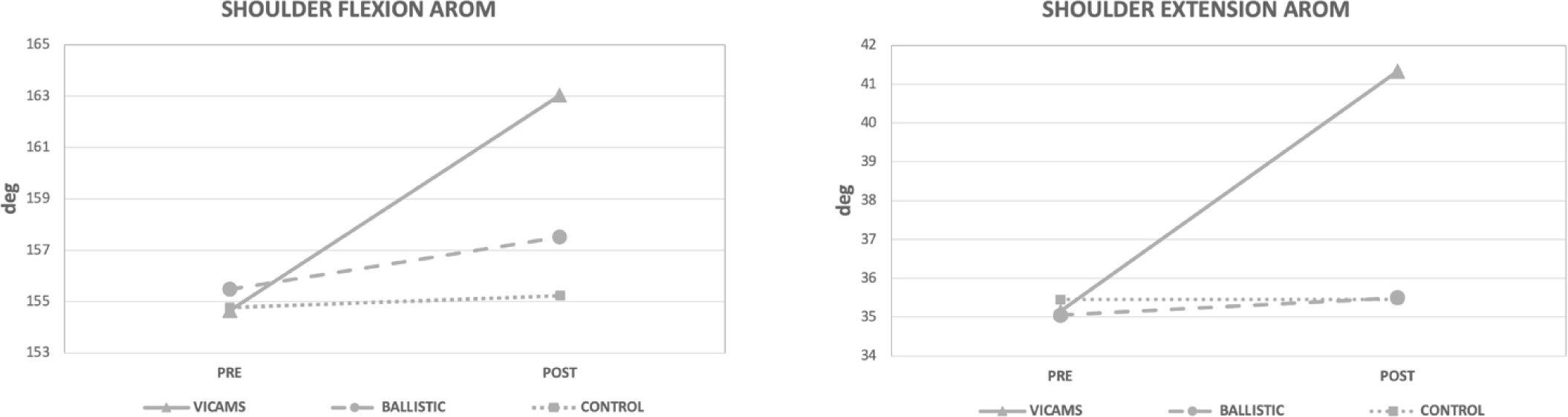
AROM: In the SF, intra-group differences were observed in both shoulders in the VICAMS group by increasing the values compared with the initial values (p < 0.001). On the right shoulder, the mean AROM increased from 154° to 163° (5.34%), while it increased from 155° to 163° (5.49%) on the left shoulder. Additionally, the BS group showed increased baseline values in the right (1.22%, p < 0.001) and left (1.38%, p = 0.001) shoulders. Between-group differences were observed for the VICAMS group after the intervention (Figure 3), with statistically higher values in the right (p = 0.014) and left (p = 0.018) shoulders than in the BS group and in both shoulders compared to the CG (p < 0.001). For SE Arom, intra-group differences were observed in both shoulders as values increased compared to baseline values for the VICAMS group (p < 0.001) and BS group (p = 0.002). In the VICAMS group, the mean AROM increased from 35° to 41° (17.57%) in the right and left shoulders. Between-group differences were observed in the VICAMS group after the intervention, with significantly higher AROM values in the right shoulder than in the BS (p = 0.006) and CG (p = 0.002) groups and higher values in the left shoulder than in the BS (p = 0.018) and CG (p = 0.035) groups (Figure 3).
Figure 3
Pre and postdifferences between groups. Mean active range of motion (ArOM) values (º) for shoulder flexion and extension
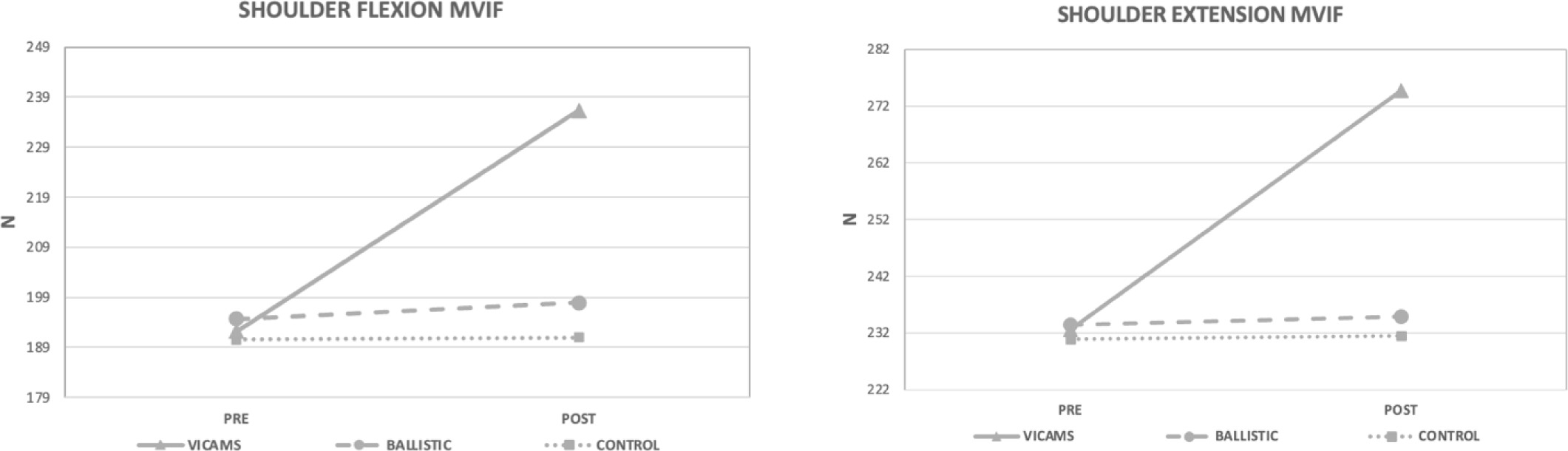
MVIF: In terms of SF, intra-group differences were observed in both shoulders in the VICAMS group, with higher values compared to baseline (22.96%,p < 0.001). the BS group showed an increase in the right shoulder (2.13%, p = 0.005) but not in the left shoulder (1.19%, p = 0.66) compared to the baseline values. Between- group differences showed that the VICAMS group had significantly higher MVIF values in the right shoulder after the intervention compared to the CG (p = 0.028) but not in the BS group (p = 0.111) (Figure 4). In the left shoulder, these values were not statistically significant (p > 0.05). For SE MVIF, intra-group differences were observed in both shoulders in the VICAMS group, with higher values compared to baseline values (18.04%, p < 0.001). the BS group showed an increase in the right shoulder (1.21%, p = 0.044) but not in the left shoulder (0.04%, p > 0.05). No significant differences were observed between the groups (p > 0.05) (Figure 4).
Figure 4
Pre and postdifferences between groups. Mean maximal voluntary isometric strength (MVIF) values (newtons) for shoulder flexion and extension
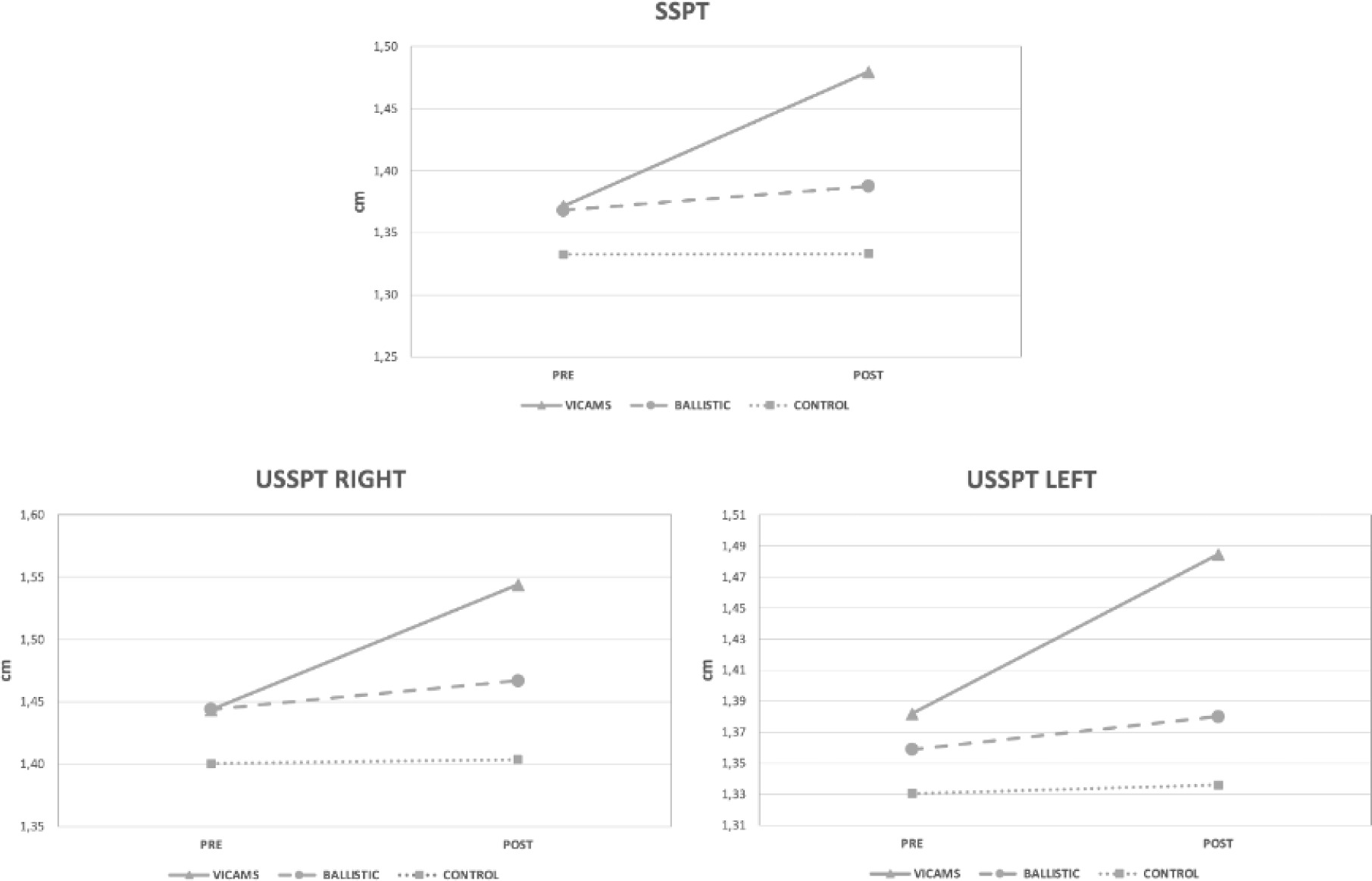
In terms of throws, intra-group differences were observed as values increased compared to baseline in both the VICAMS and BS groups (p < 0.001). In SSPT, the average throw distance increased from 1.37 to 1.48 m (7.87%) after VICAMS. After BS, the distance increased from 1.37 to 1.39 m (1.43%). In the one-handed throws, the mean distance increased from 1.44 to 1.54 m in the right arm (6.96%) and 1.38 to 1.48 m in the left arm (7.42%) after VICAMS. After BS, the average distance increased from 1.44 to 1.47 m in the right arm (1.59%) and 1.36 to 1.38 m (1.55%) in the left arm. No significant differences were found between the groups (p > 0.05) (Figure 5).
Discussion
The study compared the acute effects of BS and VICAMS on Arom, MVIF, USSPT, and SSPT variables. One of the most important findings was that, compared to BS, VICAMS generated acute improvements in AROM and MVIF of the shoulder and increased throwing distance in the SSPT and USSPT. Although both showed improvements across all variables, the VICAMS was superior to BS. These results demonstrate the efficacy of alternative and effective strategies for improving strength and athletic performance.
AROM improvements were observed after BS, which is in line with other studies showing an immediate improvement in flexibility after BS [29-31]. However, the studies used procedure durations of 15 s [30], 30 s [31], and 1 min [29], while our study used 20-second periods. Despite numerous investigations on the acute effects of BS on flexibility [32], it has not been studied specifically on the shoulder joint, with the vast majority focusing on the lower body. In any case, the increase in the range of motion after BS is justified by the decrease in resistance to stretch by increasing muscle temperature [33]. Another factor that could improve flexibility following BS is an increase in the subject’s tolerance to stretch tension [34].
Regarding the AROM improvement VICAMS, the fact that flexibility is not a specific objective of isometric training means that there are practically no studies on this subject. We have to go back to Hartley-O’brien [35] and Hardy [36], who found significant improvements by performing active stretching of the hip using an external counter force and holding the position for 6 s at the end of the movement. They also found significant improvements of more than 15° in AROM after three weeks of intervention. We established similar points in our study, in which the shortening position was maintained for 5 s by activating the agonist muscles without applying an external counter force and for much longer. The improvements in AROM after VICAMS are understood because isometric contractions of the agonist muscles and the consequent decrease in antagonist tension by reciprocal inhibition [12, 37] is a good way to improve active flexibility [35, 36]. This coincides with the results of the present study and suggests that VICAMS may be useful in acutely improving AROM.
Superior improvements were found in maximal isometric strength after VICAMS. Likewise, improvements were found after the application of BS, in agreement with studies affirming the positive effects of BS on sports performance [38]. Hough et al. [38] explained that these improvements were due to increased neuromuscular activity, which they recorded through electromyography (EMG). In addition, post-activation potentiation (PAP) and temperature increase after BS favour strength development [13].
As mentioned above, the literature linking shoulder BS and maximal strength is nonexistent. the closest work is that of beedle et al. [39], who found that dynamic (non-ballistic) diagonal shoulder stretching did not affect one repetition maximum (1RM) bench press performance. Participants performed three sets of 30 s on each shoulder, a much lower volume of work than in our study, which probably justifies their results. On the other hand, a few studies on isometric shoulder training focussed on strength improvement for rehabilitation, not on performance. Hagberg et al. [8] and his team used isometric contractions of the shoulder at 90° of flexion in sets of 5 s and found it to improve strength, which coincides with the five-second sets used in our study. Some studies have associated these increases with neural factors [40] and an increase in PAP [41]. Furthermore, maximal isometric strength improvements have been found following isometric training at short muscle lengths [10]. In addition, bandy et al. [9] applied isometric contractions in short knee joint positions (30°) and achieved strength improvements. In both cases and in contrast to our study, training was applied to the lower body after several weeks of training and did not reach maximal shortening. As such, if the results of the application of BS are contrasted with VICAMS, the higher levels of improvement in MVIF can be justified since isometric contractions at short muscle lengths produce less fatigue [42], and shorter muscle lengths produce more neural activation [6]. therefore, VICAMS may be an effective acute method of increasing muscle strength.
There were significant intra-group improvements in throwing ability after BS and VICAMS, although not in the post hoc between-group analysis. Several studies have found improvements in weighted throw performance after ballistic training [43]. bellar et al. [43] and their team found acute improvements following shot-put training with loads above the competition level and found that PAP was the main cause of increased performance. Although the present study used body weight as the ballistic stimuli, the potentiation component was similar. the beneficial mechanisms of PAP are widely known in the literature [41]. In addition, increased EMG activity after BS suggests greater stimulation of the nervous system by increasing heart rate and temperature to optimal levels [33]. Other studies have also found improvements after 12 weeks of ballistic exercises involving the throwing of medicine balls [44]. Indeed, Kontou et al. [45] investigated acute throwing improvement after isometric shoulder training involving six-second isometric pushups. the results indicated that these exercises are potent methods for increasing throwing performance, which is consistent with the findings of the present study. Several studies have also shown improvements in SSPT [26] and USSPT [46] after shoulder strength training, with the results primarily justified by increased peak power due to the PAP mechanism [47]. based on these results, VICAMS could be considered a good method for improving acute throwing performance.
The results of this study provide valuable information that could provide coaches with new resources to achieve immediate improvement in shoulder performance. there are many sports in which shoulder muscle activation is crucial for optimal performance, such as swimming, baseball, basketball, and volleyball, and the knowledge gained here could be applied easily, quickly, and economically, both in pre-competition warm-ups and training. Furthermore, these results can contribute to advances in rehabilitation by providing an alternative to commonly used techniques [48]. Indeed, shoulder dysfunction is one of the leading causes of musculoskeletal pain and affects approximately 2030% of the general population [49]. Improving flexibility and strength could help to improve these conditions.
TMs research pioneered the study of the acute effects of shoulder training on maximally shortened muscle positions. Previous work by our group found similar results for the lower limbs [50]. Moreover, other authors studied the acute effects in positions close to maximal shortening and showed improvements in lower limb strength [9, 10].
Performance and measurement variables were controlled thoroughly, though the study was not without its limitations. First, the results cannot be extrapolated to athletes because of the participant's profiles, though they were more interesting because they reflected a large proportion of the population. Future studies should focus on the acute effects of VICAMS on athletes, as this would be interesting for coaches. In addition, future studies on the differences between males and females could be worthwhile due to the physiological characteristics of force production. Furthermore, future research should study the chronic effects of VICAMS, which will provide insights into the duration of the response and its long-term implications. Another limitation is the need for external resistance, and it remains to be determined how another type of resistor may influence whether the participant performs the VICAMS independently. Nonetheless, coaches could assist the athlete and assess the quality, speed, and quantity of the force applied. Finally, a future line of research on the application of VICAMS in rehabilitation could explore improvements in muscle and joint function.
Conclusions
Applying VICAMS to the shoulder can acutely improve active flexibility, maximal strength, and throwing ability in physically active subjects. In this homogeneous group, all variables obtained the best results compared to traditional training methods such as BS. Coaches should consider using VICAMS as part of a warm-up protocol or an immediate performance-enhancement strategy. A short period of time is required to perform nine contractions of 5 s for each of the shoulder movements. As such, it represents a fast, effective, and low-cost practical application, which could benefit many sporting practices, as most sports require active flexibility and upper-body strength. therefore, our findings indicate that a new way of working in physical preparation could be developed.