Introduction
Online gaming is an Internet-based activity using electronic devices such as smartphones, computers, or laptops, enjoyed by people of all ages, including children, teenagers, and adults [1]. ‘E-sports enthusiasts’ does not refer to gaming competitions, but to the individuals who are passionate about or engaged in them. These athletes typically practice or compete using smartphones and have injury profiles similar to office workers due to prolonged sitting. Professional E-sports athletes often train 4–10 hours daily, with extended hours during tournaments reaching 8–10 hours [2].
According to the Indonesian Internet Service Providers Association (APJII) 2021–2022 survey, 77.02% of Indonesians, or approximately 210.03 million people, have access to the Internet, placing Indonesia among the top 20 countries for Internet usage in gaming. In 2022, 89.03% of Indonesians were smartphone users, with 83.48% being Internet users, and 19% of smart-phone users were E-sports enthusiasts. According to Wahyuni and Putra [1], in 2018, Indonesia ranked among the top 4 countries globally with over 100 million active smartphone users. Research by Arthamevia et al. [3], based on a 2021 digital report, shows that 60.2% of gaming activities in Indonesia were conducted via smartphone, with an average usage of 1 h and 16 min per day for gaming.
Digital gaming addiction has negative impacts, including laziness in completing tasks and discomfort when not playing, which can lead to abusive behaviour in some individuals [1]. Excessive smartphone use increases dopamine levels, posing health risks [4]. Prolonged smartphone use causes addiction and several issues for physical, psychological, social, familial, and educational issues [5].
Headache is an uncomfortable sensation in the head, occurring unilaterally or bilaterally, and may radiate to the face, eyes, jaw, and neck. The World Health Organization (WHO) reports that the global prevalence of headaches is 47%, with the highest proportion caused by tension-type headaches (38%), followed by migraines (10%) and chronic headaches (3%) [6]. Data indicate that 40% of adults aged 18–65 years experience headaches. E-sports enthusiasts with playtimes exceeding 6 h force their brains and eyes to work harder, increasing the risk of headaches [4].
Headaches are prevalent among and E-sports enthusiasts due to prolonged fixed head positions, prolonged static sitting postures, mental stress from competitive pressure, and intense focus [7]. E-sports activities, which demand physical and mental skills, increase enthusiasts’ susceptibility to these headaches.
The craniovertebral angle (CVA) is used to evaluate head posture. Research shows that a reduced CVA is linked to forward head posture (FHP), which can cause headaches due to upper cervical ischemia and increased posterior cervical muscle tone [8]. FHP also leads to neck musculoskeletal tension and pain, further triggering headaches. Studies indicate that weakened c1–c3 cervical nerve roots can release irritants into joint capsules, ligaments, and the spine, worsening symptoms [9]. Additionally, suboccipital muscle pain points are closely correlation with referred pain in the occipital and temporal regions, emphasising their role in the pathophysiology of headaches [10]. Additional factors, including anxiety, high radiation exposure, and poor posture, are recognised as headache triggers by increasing ischemia in the neck and head muscles. Static postures, such as prolonged head bowing, can aggravate headaches by causing excessive muscle contractions and reduced blood and oxygen flow to the brain [4].
The previous study also showed that prolonged gaming may increase the risk of headaches when exposed to high radiant light beams. This exposure affects a group of retinal cells, such as rods and cones, that are important for light perception and regulating sleep cycles. The research results by Rori et al. [7] show that neurotransmitters in retinal cells can affect neurons involved in the headache mechanism.
Few studies have found a correlation between digital gaming addiction, playtime, and CVA with headache symptoms in E-sports enthusiasts. A previous study only focused on smartphone addiction in E-sports enthusiasts; few studies highlight how smartphone addiction and playtime can be related to headaches in E-sports enthusiasts. This study also examined types of devices other than smartphones, such as computers and consoles, and specifically explored the correlation between CVA and headaches, whereas research from previous studies only discusses the correlation between CVA and neck pain [11]. Therefore, the aim of this study is to determine the correlation between digital gaming addiction, playtime, and CVA with headache symptoms in E-sports enthusiasts. This research is expected to be baseline data to form the basis of developing preventive programs for E-sports enthusiasts and training programs to improve performance and prevent injuries.
Material and methods
Research design
This research design is observational research with a cross-sectional study approach that aims to determine whether the level of digital gaming addiction, playtime, and CVA contribute to headache symptoms in E-sports enthusiasts.
The variable consists of the dependent variable, headache symptoms, and the independent variables, digital gaming addiction, playtime, and CVA.
Sampling
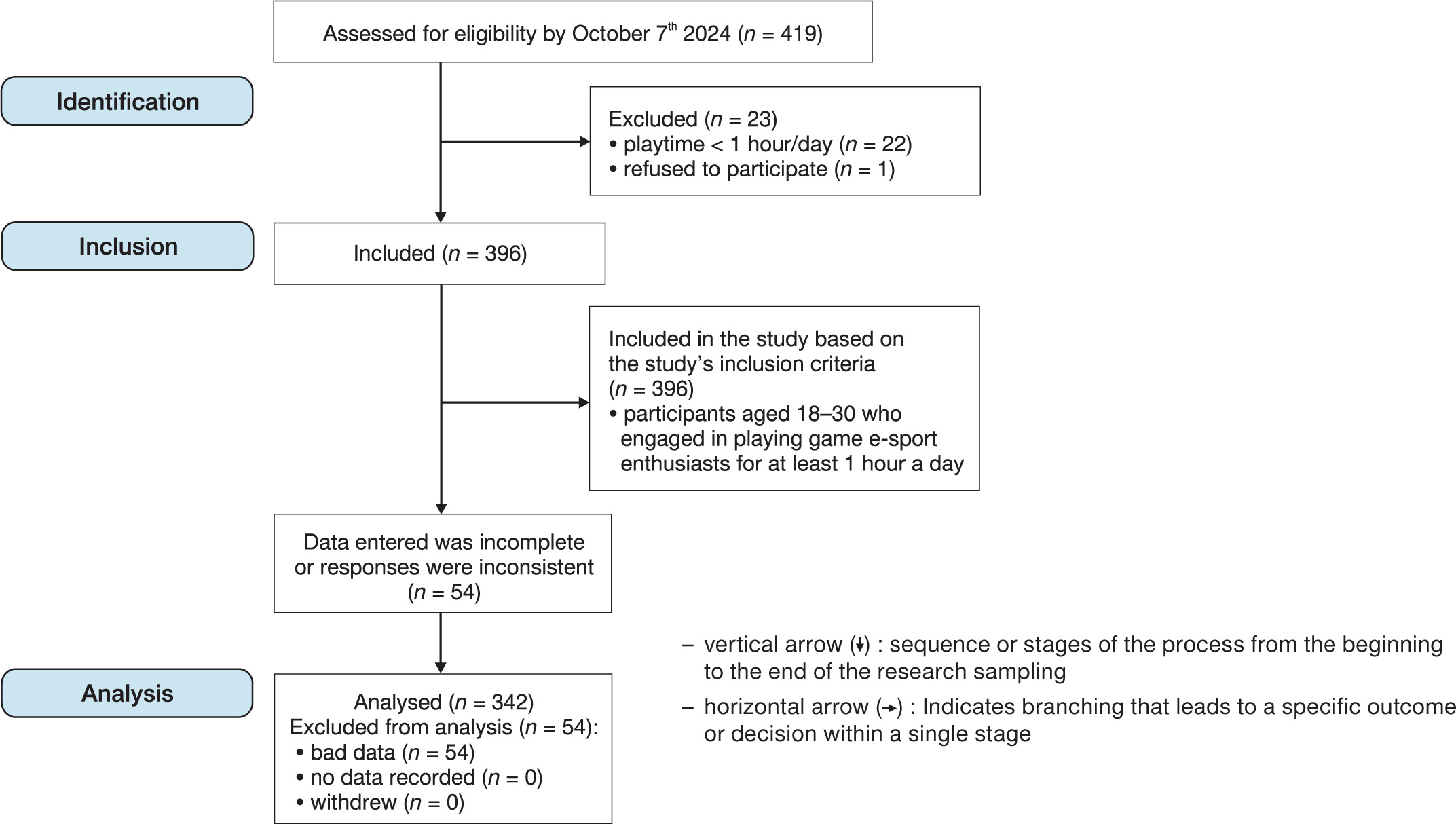
The sampling technique employed in this study was non-probability sampling with an accidental sampling technique. The population in this study is unknown Indonesian E-sports enthusiasts. The sample size in this study was determined using the Lemeshow formula, which is commonly used to calculate samples in large or unknown populations. In this study, the estimated maximum proportion of events was 30%, with a tolerable error rate of 5%. Based on calculations using the Lemeshow formula, a sample size of 342 respondents was obtained. This number is considered sufficient to represent the population and produce valid and reliable data. The research was conducted offline and online from October to December 2024 using a virtual platform. A total of 419 E-sports enthusiasts expressed an interest in filling out the research questionnaire. After going through the data screening process, 342 respondents who fit the inclusion criteria were obtained (Figure 1).
Sample criteria
The inclusion criteria in this study are: 16–30 years old, male or female, semi-professional, professional or amateur who play video games ≥ 1 hour/day, actively playing video games > 6 months, and willing to become respondents. Exclusion criteria in this study included a previous history of musculoskeletal injury to the fingers, wrists, hands, elbows, shoulders, or back in the last < 6 months that were not related to gaming activities and having other medical disorders that may affect the results of the study, such as neurological disorders like carpal tunnel syndrome, and wrist drop and autoimmune diseases.
Operational definition of variables
Headache is a common condition characterised by facial, neck, and head pain. Its severity can be measured with the Headache Disability Inventory (HDI): mild (0–20), moderate (21–40), severe (41–60), and very severe (61–100). Digital gaming addiction is the dependence on using smartphones excessively and is assessed with the Video Game Addiction test (VGAT): not addictive (0–14), less productive (15–29), moderate (30–42), and severe (43–54). Playtime is the length of time it is used to play online games [12]. This measurement is classified into low playtime (< 3 h), moderate (3–7 h), and long (> 7 h) by asking the question ‘How long do you play games in a day?’ [12]. The CVA is the angle between the head and neck, measured using photographs analysed with the Kinovea software (Figure 2). Measurements were conducted by the assessor rather than the participant to ensure consistency and accuracy.
Figure 2
Illustration of individual gaming posture measurement based on primary data, using the Kinovea application

The measurement of CVA in this study was carried out using the lateral photographs-based posture analysis method using the Kinovea application. The data collection procedure was conducted as follows:
1. Participants are asked to stand or sit in a neutral and relaxed position with their gaze straight ahead and to relax their shoulders to prevent tension that could affect the measurement.
2. A digital camera was positioned laterally at a fixed distance of 1.5 metres and a height corresponding to the participant’s tragus to capture sagittal views of the participant’s head and neck [13].
3. The photographs were then analysed in Kinovea to determine the angle between the horizontal line at the spinous process of the C7 and the line extending to the tragus of the ear. The classifications used were normal (≥ 50°), mild (45.5–49.9°), and moderate-severe (< 45.5°).
An illustration of the individual playing posture measurement settings can be seen in Figure 1. This study also evaluated differences in headache symptoms between smartphone, computer, and console users without measuring a direct correlation between the type of device used and headache symptoms.
Data analysis
This research data analysis employed IBM SPSS Statistics version 30 to conduct univariate analyses to determine descriptive data, bivariate analysis using Spearman’s rank correlation test to determine the correlation between the independent variables and the dependent variable, and multivariate analysis with ordinal regression test to determine the contribution of the independent variables that correlate with the dependent variable.
Results
This study aims to determine whether the level of digital gaming addiction, playing time, and CVA contribute to the occurrence of headache symptoms in E-sports enthusiasts. The flowchart in Figure 1 provides a visual representation of the assessment of the respondents’ eligibility for this study as a guide for conducting the statistical analysis of the subjects who completed the research stages’.
During the initial recruitment phase, which commenced on 7 October 2024, a total of 419 people were evaluated for eligibility to participate in the study. Of these, 23 people were eliminated because 22 people did not meet the criterion of playing duration of at least one hour per day, and one person refused to participate, leaving 396 people who met the inclusion criteria. The inclusion criteria included ages between 18 and 30 years old and actively involved in esports gaming activities with a minimum duration of one hour per day. Following the data validation process, 54 participants were excluded due to incomplete or inconsistent data with the research instrument. As a result, 342 participants with complete and valid data were included in the final analysis and proceeded to the follow-up stage of the study.
Table 1
Demographic characteristics of respondents
The demographic characteristics of the respondents are summarised in Table 1. In this study, a total of 342 E-sports enthusiasts who met the inclusion criteria were included after completing the research questionnaire and passing the data screening process. The data was then tested for normality, and the results showed that the data was not normally distributed. There was a significant age difference, with the majority of respondents aged 16–20 years (74%, n = 253), E-sports participation as amateur (recreational) (71.6%, n = 245), duration of engagement ≥5 years (51.2%, n = 175), and using mobile devices (79.8%, n = 273). The other characteristic of the respondents was gender, which was 67.3% male (n = 230) and 32.7% female (n = 112).
Table 2
Statistics on descriptive characteristics of respondents
Table 3
Bivariate, regression, Kruskal–Wallis, and post-hoc analysis
| Variable | Headache | ||||
| Spearman correlation | ordinal regression | ||||
| sig. (p) | r | sig. (p) | pseudo R2 | ||
| Digital gaming addiction | 0.001 | 0.357 | 0.001 | ||
| Playtime (h/day) | 0.511 | –0.036 | – | 0.001 | 13.3% |
| CVA | 0.004 | –0.155 | 0.078 | ||
[i] Digital gaming addiction (p = 0.001) and CVA (p = 0.004) were significantly correlated with headache symptoms, while playtime was not (p = 0.511). Ordinal regression indicated that these two variables contributed 13.3% to headache symptoms. The Kruskal–Wallis test was applied to assess differences in headache symptoms based on device type (smartphone, computer, console) and duration of engagement (≥ 6 months, ≥ 2 years, ≥ 5 years), due to the non-normal data distribution. No significant differences were found (device: p = 0.279; duration: p = 0.327). Post-hoc analysis confirmed that no pairwise comparisons showed significant differences.
The descriptive statistics of the respondents are summarised in Table 2. Digital gaming addiction in most respondents was in the unproductive category 15–29 (56.4%, n = 193). Playtime in most respondents was the low category (< 3 h/day), amounting to (45.9%, n = 157), with an average of playing 2 h/day. CVA in most respondents was in the regular category (59.6%, n = 204), and headache symptoms experienced by respondents were primarily in the mild category (38.3%, n = 131).
Based on the results in Table 3, the bivariate and regression analyses showed that digital gaming addiction (p = 0.001) and CVA (p = 0.004) were significantly correlated with headache symptoms in E-sports enthusiasts, while playtime (p = 0.511) showed no significant correlation. Based on the correlation coefficient (r), digital gaming addiction had an r-value of 0.357, indicating a moderate positive correlation with headache symptoms that was statistically significant. In contrast, playtime had an r-value of –0.036, reflecting a weak negative correlation that was not statistically significant. Meanwhile, CVA showed r = –0.155, indicating a weak negative correlation that was statistically significant. Although digital gaming addiction and CVA demonstrated statistical significance, the strength of their correlation remains weak. The results of the ordinal regression test in the regression Analysis table show that the digital gaming addiction variable and the CVA, if tested simultaneously, have a significant contribution (p = 0.001) of 13.3%. In comparison, the remaining contribution of 86.7% is influenced by other variables not examined in this study. Digital gaming addiction contributed the most to this 13.3% (p = 0.001) compared to CVA (p = 0.078).
The analysis of differences between groups based on the type of device used and engagement duration in play activities was conducted using the Kruskal–Wallis test. The results showed that there was no significant difference between the device type groups (p = 0.279) or the engagement duration groups (p = 0.327) on headache symptoms. However, to strengthen the analysis, a post-hoc test was conducted. The results of the post-hoc test showed that there was no significant difference between each pair of groups, either in device type (smartphone vs computer, p = 0.977; computer vs console, p = 0.419; smartphone vs console, p = 0.247) or in length of engagement (≥6 months vs ≥ 2 years, p = 0.952; ≥ 2 years vs ≥ 5 years, p = 0.508; ≥ 5 years vs ≥ 6 months, p = 0.392). This indicates that neither the device type nor duration of engagement made a significant difference to the headache symptoms experienced by respondents. Overall, the results of this study suggest that the level of digital gaming addiction and head posture (CVA) have an important role in headache symptoms, while the duration of play, device type, and duration of engagement did not show statistically significant relationships or differences.
Detrended normal Q–Q plots of playtime distribution, digital gaming addiction distribution, craniovertebral angle (CVA) distribution, headache distribution
Based on primary data from the statistical analysis, the following results were obtained: Figure 3 [distribution of digital gaming addiction levels (digital gaming addiction distribution)] – this figure illustrates the distribution of digital gaming addiction levels among respondents based on VGAT scores; most respondents fall into the ‘less productive’ category, followed by the ‘non-addictive’ category, with only a small portion in the moderate and severe categories; Figure 4 [distribution of playing duration (playtime distribution)] – this figure shows the distribution of respondents based on their daily gaming duration; the majority of respondents reported playing less than 3 h per day (low category), followed by respondents with moderate duration (3–7 h), and only a small portion who played more than 7 h per day (high category); Figure 5 (headache severity distribution) – this figure displays the distribution of headache severity among respondents based on HDI scores; most respondents experienced headache symptoms in the mild-to-moderate category, while a small proportion experienced severe to very severe headaches; Figure 6 [craniovertebral angle (CVA) distribution]– this figure presents the classification of craniovertebral angles (CVA) among respondents; the majority have normal CVA (≥ 50°), while the rest are divided into the mild (45.5–49.9°) and moderate–severe (< 45.5°) groups, indicating a tendency towards forward head posture.
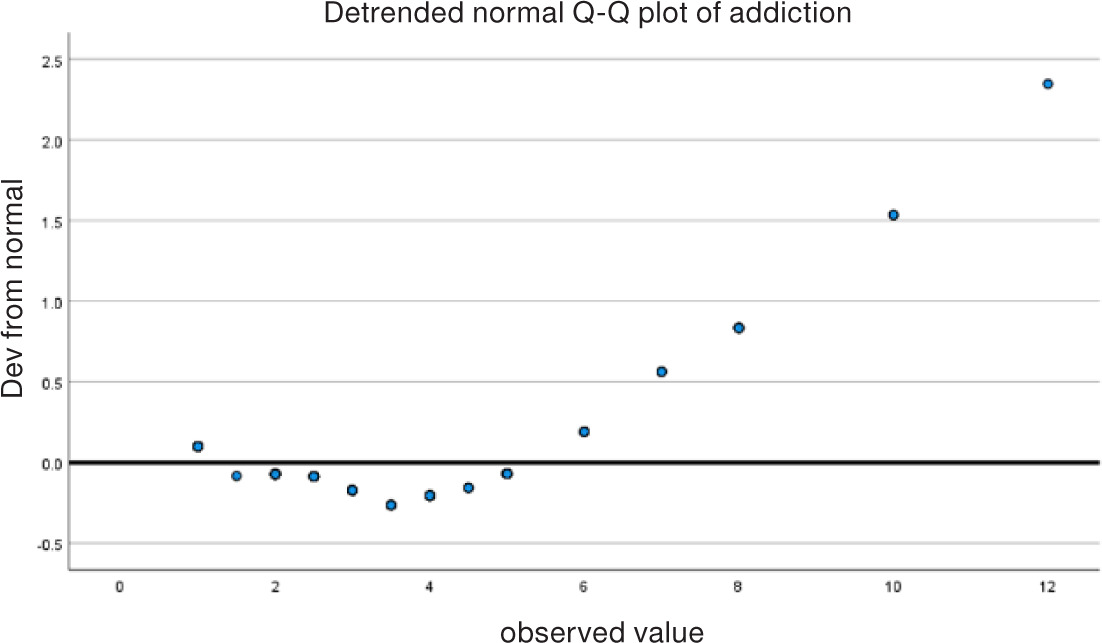
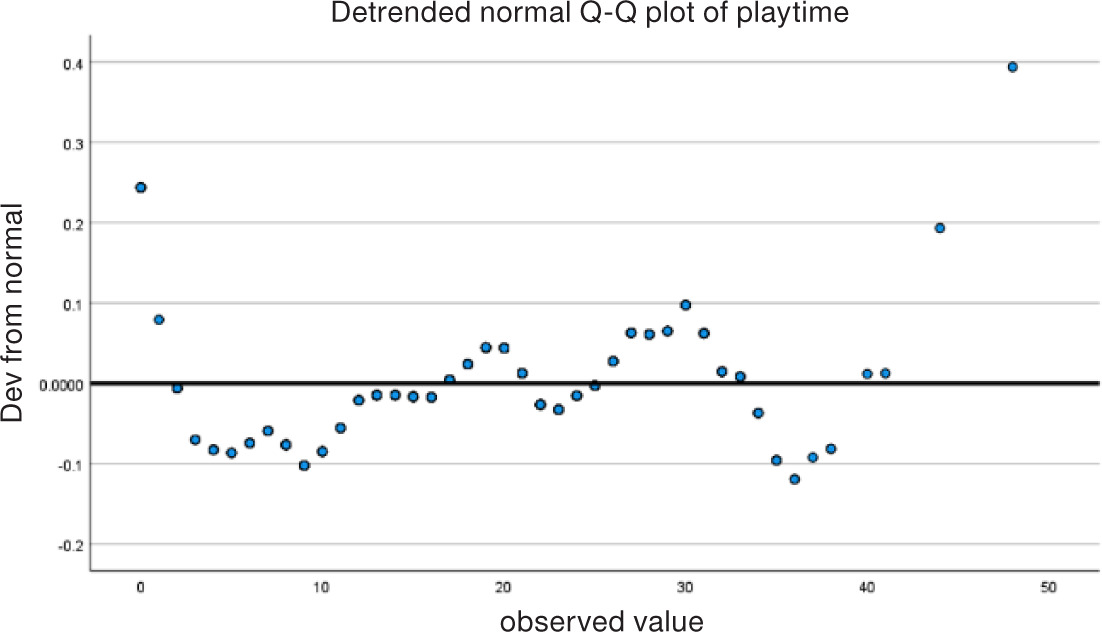
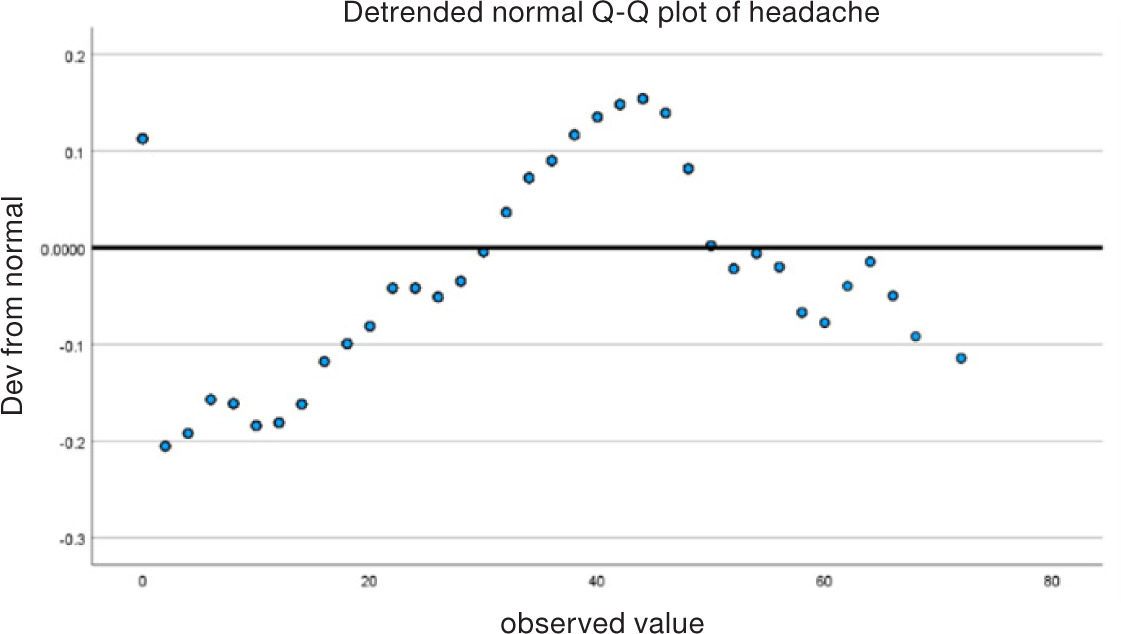
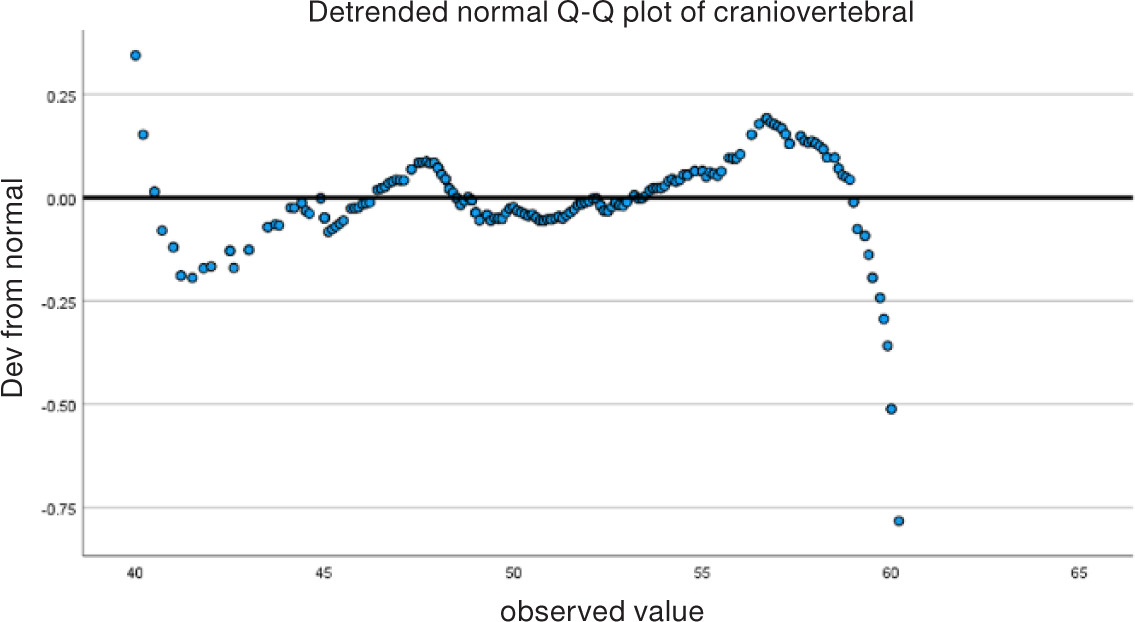
Data normality was assessed using detrended Q–Q plots. As shown in Figures 3–6, the data did not follow a normal distribution, thus supporting the use of non-parametric statistical tests such as Spearman’s correlation and Kruskal–Wallis analysis.
Discussion
This study examined the contribution of digital gaming addiction, playtime, and CVA to headache symptoms in E-sports enthusiasts. Digital gaming addiction had a moderate effect, while playtime showed no significant impact, and the CVA was within the normal range. This study investigated the correlation between the independent variables and headache symptoms using a cross-sectional design with accidental sampling, analysed through Spearman’s rho correlation and ordinal regression tests. The sample size was 342 people, consisting of amateur, semi-professional, and professional E-sports enthusiasts, which represented a representative population in Indonesia.
Digital gaming addiction had a moderate effect on headache symptoms, as supported by tariq et al. [14], who found that excessive gadget use triggers headaches despite normal CVA. Falkenberg et al. [15], revealed that ergonomic factors and screen lighting also contribute to the emergence of headaches. He also highlighted that smartphone screen radiation due to playing games can affect brain function, which can ultimately trigger headache symptoms. Meanwhile, a long duration did not contribute to headache symptoms in E-sports enthusiasts, possibly due to the low average playing time of the E-sports enthusiasts studied. This study aligns with previous research findings that show a correlation between digital gaming addiction and headache. Meanwhile, Pratama and Suherman [16] found that digital gaming addiction increases the frequency of headaches, particularly among adolescents. Kartika et al. [4], reported that game addiction can cause headaches due to reduced physical activity and increased muscle tension. As noted by Apriyeni et al. [17], digital gaming addiction is correlated with headaches, as it causes sleep disturbances when playing games before bed, reducing concentration and triggering headaches.
The CVA plays a role in headache symptoms, but a normal CVA value does not guarantee the absence of headaches. Poor posture, such as FHP, leads to upper-crossed syndrome and altered alignment of the cervical and thoracic vertebrae [2]. Lin et al. [18], found that FHP had a correlation with reduced CVA and limited cervical range of motion, especially in long-sitting gamers. Lee and Lee [10], reported that reduced CVA aggravated headaches compared to healthy individuals. FHP patients have weakened neck muscles, including deep flexors and extensors. Cervical stabilisation exercises are recommended to improve neck muscle endurance, normalise cVA, and reduce headache symptoms [19].
This study did not find a significant correlation between gaming duration and headache symptoms. This finding contradicts some previous studies, which showed that gaming for more than three hours can trigger headaches [7, 20]. One possible reason for this difference in results is that the average duration of gaming among the respondents in this study was only 2.9 hours, which is still below the 3-hour threshold, which may not be enough to trigger the headache symptoms found in previous studies. In addition, Zafira et al. [6], noted that smartphone use exceeding 10 times a day or 60 min of gaming time significantly increased the risk of headaches. Research by Gupta et al. [21], showed that 47.4% of respondents who used a smartphone for 7–10 h every day experienced headaches, which is consistent with research showing that use of more than 2 h every day is not ideal.
This indicates that the duration of gameplay alone may not be a major factor in causing headaches. Instead, other factors such as the player’s posture, suboptimal ergonomics, poor screen lighting, and the level of addiction to digital games may have a more substantial impact on headache symptoms. Apriyeni et al. [17], noted that playing games before bedtime leads to poor sleep quality and headaches, while Falkenberg et al. [15] highlighted that prolonged exposure to smartphone screen radiation during gameplay can affect brain function and trigger headaches. Despite this supporting evidence, the present study found that gameplay duration alone did not significantly contribute to the reported symptoms.
The absence of a significant correlation in this study may also be due to respondent bias, where participants may have inaccurately reported their gaming duration, resulting in data that falls below the three-hour threshold, which previous studies have identified as a critical point for headache onset. Furthermore, limitations in the measurement of the CVA using the Kinovea application (ICC 0.929–0.995) may have influenced data accuracy due to poor-quality photographs or difficulty identifying anatomical points. In addition, respondent bias in reporting game-play duration may produce results that are less representative of the actual condition.
Overall, this study confirms that digital gaming addiction has a correlation with headache symptoms, especially headaches. A normal CVA does not always guarantee the absence of headache symptoms because postural factors such as FHP still have the potential to cause biomechanical changes in the cervical vertebrae, which can trigger headaches. Meanwhile, the shorter duration of playtime compared to other studies is likely the reason for the absence of a significant correlation between playtime and headaches in this study. In addition, this study analysed the differences in headaches on each device, such as smartphones, computers, and consoles, finding that this was correlated with headaches in E-sports enthusiasts. The higher prevalence of headaches among smartphone users may correlate with factors such as prolonged neck flexion, increased screen exposure, and a less ergonomic posture compared to computers and consoles [22].
Headache disorders resulting from digital gaming addiction and CVA abnormalities in E-sports enthusiasts are a concern in the healthcare sector, particularly in the field of physiotherapy. Poor posture and prolonged playtime increase the risk of headache symptoms in E-sports enthusiasts, thus emphasising the important role of physiotherapy in preventing and reducing headaches and CVA-related symptoms correlated with FHP [10]. Physiotherapists can integrate gaming addiction screening into evaluating headache complaints, while an interdisciplinary approach to physical activity can help reduce addiction and headache symptoms. Postural interventions, such as cervical stabilisation exercises, address muscle imbalances and restore the CVA to normal, preventing headaches due to upper-crossed syndrome [19].
This finding may influence clinical physiotherapy practice by encouraging the development of prevention, education, and exercise programs. CVA measurements can be included in routine examinations to detect FHP and prevent headaches through postural and neck stabilisation exercises. In addition, exercise therapy focused on neck stabilisation can be recommended to address this issue. Health promotion efforts, such as educating E-sports enthusiasts about ergonomics, such as proper screen positioning, ergonomic chairs, and regular breaks every 30–60 min, can prevent neck strain and headaches. Stretching exercises for the neck, shoulder, and back flexors can relieve muscle tension and improve circulation [23].
The impact on daily life includes adopting a healthy lifestyle by reducing gaming time, improving posture, exercising regularly to maintain neck and back fitness, and avoiding gaming before bedtime to prevent sleep disturbances and headaches. This study highlights the risks of gaming addiction and poor posture, which can be socialised through social media, schools, and health centres. Its strength lies in addressing the gap in the literature on digital gaming addiction, playtime, and the CVA’s correlation with headaches.
The study’s limitations include technical challenges in measuring the CVA using the Kinovea app due to unclear photographs or difficult-to-identify anatomical points, affecting data accuracy and head posture measurement validity. Additionally, the low and less variable reported playtime may be influenced by respondent bias, where participants are reluctant to report actual playtime, affecting the study’s results.
These issues can impact conclusions regarding the correlation between head posture, playtime, headache symptoms, and the reliability of posture intervention recommendations. The correlation could have been stronger if the reported data were more accurate. However, the generalisability of the results is limited by focusing only on E-sports enthusiasts and the need for greater variability or variation in the inclusion criteria. The accidental sampling technique aids in meeting inclusion criteria and maintaining data validity, while Spearman’s rho and ordinal regression effectively evaluate correlations and variable contributions.
Future studies should use more appropriate questionnaires or tools for CVA measurement and should implement standardised procedures, such as ensuring proper lighting, consistent photograph-taking angles, and clear instructions to improve measurement accuracy. To minimise measurement bias, all CVA analyses were performed by a trained researcher, and each measurement was repeated twice to ensure reliability. If there was a difference of more than 1° between two measurements, a third measurement was taken, and the average value was used for analysis. Additional variables, such as the type of device used (smartphone, computer, or console), participation in E-sports (amateur, semi-professional, professional), and duration of professional involvement, may provide more comprehensive insights. Studies on professional E-sports teams are also recommended to better understand the factors that influence headache symptoms and to design more effective prevention programs to minimise injuries and improve the performance of E-sports enthusiasts.
Conclusions
The results demonstrated that moderate levels of digital gaming addiction and normal CVA contributed to headache symptoms in E-sports enthusiasts, while low playtime had no effect. However, the average playing time reported in this study was not sufficient to trigger headache symptoms. Nevertheless, If the playing time is extended to moderate or high levels, the risk of headaches increases. In addition, the type of device also affects the occurrence of headaches, with smart-phone users experiencing the highest rates of headaches compared to computer and console users. Factors such as posture while gaming, age, E-sports participation, duration of professional involvement, gender, and exposure to light from device screens may also influence the onset of headaches.