Introduction
Children in the preadolescent and early adolescent stages are particularly susceptible to musculoskeletal adaptations due to rapid growth and the maturation of postural control mechanisms. Although several studies suggest that carrying a schoolbag may influence postural development, especially in the cervical and shoulder regions, the evidence remains inconsistent [1, 2]. During this developmental period, numerous biomechanical and hormonal changes require efficient motor adaptation [3], increasing the likelihood of compensatory strategies emerging in response to external load [2].
Despite guidelines recommending that schoolbag weight remain within 10–15% of a child’s body weight, younger schoolchildren frequently exceed this threshold [4–6]. This coincides with an increasing prevalence of back and neck discomfort, with studies and reports indicating that up to one-third of children experience back pain and that most symptoms originate from the cervical spine [7]. Although school-based education programmes show promising results in improving load-handling behaviours and reducing back pain [8], the lack of longitudinal evidence limits our understanding of how these adaptations evolve over time.
Postural compensations to external load commonly manifest as deviations in the sagittal plane, including anterior trunk displacement [5] and cervical adjustments reflected in altered craniovertebral and craniocervical angles [9]. However, most available studies rely on cross-sectional designs. Only a few longitudinal investigations have examined how repeated load exposure influences postural development, and these have generally been short-term. For example, one study following children over 11 months reported increased torso rotation and abnormal kyphosis values associated with schoolbag weight [1].
Because longer-term, developmental-stage comparisons remain scarce, we conducted a longitudinal study following the same cohort of children from first to fifth grade to document changes in centre of gravity (CoG) shift and head–neck posture under load. Specifically, we examined craniocervical and craniovertebral angle adaptations over a four-year period and evaluated age-related differences in schoolbag weight, relative load, and CoG displacement. We hypothesised that carrying a schoolbag would be associated with measurable postural adaptations, including forward head posture [reflected in a decreased craniovertebral (CV) angle and an increased craniocervical (CC) angle] and shifts in CoG, and that these effects might vary by developmental stage (first vs. fifth grade) and body composition, with children of higher BMI showing more pronounced compensatory responses.
Material and methods
Subjects
The study was conducted on a sample of 60 school-children from two primary schools in Zagreb, Croatia. The same group of children was measured at two different time points: 76 children were first measured in first grade (age 7), and 60 of these children were measured again in fifth grade (age 11), resulting in a retention rate of 78.95%. Dropouts were due to relocation to a different school or illness on the day of the second measurement.
Procedure
The study was conducted using a parent questionnaire, anthropometric measurements, and kinematic analysis. The questionnaire collected basic data such as age, sex, and schoolbag-carrying habits. Height, body mass, and schoolbag weight were measured using standardised methods.
All measurements were conducted in the school gymnasium at 8:00 a.m. before the start of lessons. Each measurement session lasted approximately 10 minutes per child, and the full procedure was completed within four hours. Students were barefoot but wearing socks. The same schoolbag with a predetermined average weight was used for all participants. The average weight of the schoolbag was calculated based on the school-bags of all children included in the study. The schoolbag was then filled with books, notebooks, and school supplies to match the average calculated mass. The school-bag was a common model used, with adjustable straps, a firm backrest, and no plastic frame. The same bag and weight were used across all participants to ensure consistency. The straps were adjusted for comfort based on the children’s preferences before recording.
A total of six measurers conducted the procedures: one physiotherapist with seven years of experience, one kinesiologist with 20 years of experience (both present at both time points), and four different graduate students of physiotherapy, who assisted at different time points.
Anthropometrics
Anthropometric data included height and body mass, measured using a Harpenden anthropometer (Holtain Limited, Crosswell, United Kingdom) and a ground reaction measurement platform (Kistler Quattro Jump, Type 9290AD, Kistler Group, Winterthur, Switzerland). BMI was calculated as body mass (kg) divided by height squared (m2). The average weight of the schoolbags was determined by weighing all students’ schoolbags. All anthropometric measurements were performed according to standardised procedures [10].
Kinematics
The study measured changes in centre of gravity (CoG), CV angle, and CC angle. A Pentax K20D digital camera (Pentax, Tokyo, Japan) mounted on a tripod was used to capture videos. The camera was positioned 12 metres from the subject to capture a full-body view. Reflective markers were placed on key anatomical points, as required by the kinematic analysis software. The children stood at pre-marked positions and were measured in two conditions: without and with the schoolbag.
Centre of gravity shift
CoG shift was measured in the anteroposterior (AP) and vertical directions using the SkillSpector software (Video4coach, Odense, Denmark) [11]. The Simple Full Body digital model was used for the AP projection, and the Full Body Right Side model was used for the lateral projection. The CoG shift was calculated by tracking the movement of key anatomical points between the nobag and bag conditions. After digitising the video material and applying 2D calibration, direct linear transformation [12] was used to calculate the CoG shift. Positive AP shift values indicate forward movement, while negative values indicate backward movement. Positive vertical shift values indicate downward movement, while negative values indicate upward movement. When properly configured, the accuracy of such systems can reach up to 0.3 mm [13], with moderate-to-high interrater reliability, as indicated by intraclass correlation coefficients (ICC) ranging from 0.71 to 0.99 [14].
Craniovertebral and craniocervical angles
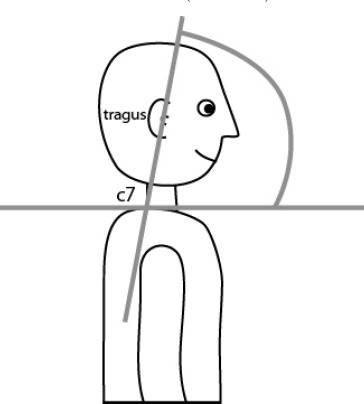
The CV angle is the angle between the line connecting the ear tragus and the C7 spinous process and the horizontal plane (Figure 1). This angle reflects the degree of head and neck flexion. The C7 spinous process was marked with a reflective marker, while the tragus was clearly visible. Measurements were taken in the lateral projection, with and without the schoolbag.
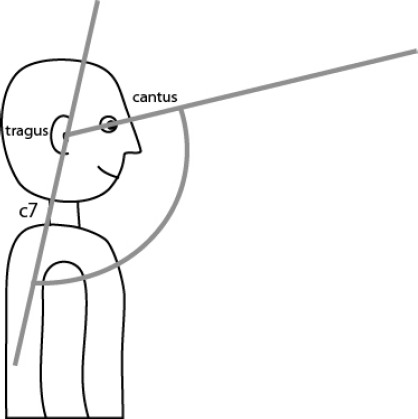
The CC angle is the angle between the line connecting the ear tragus and the C7 spinous process and the line connecting the ear tragus and the canthus of the eye (Figure 2). This angle reflects the degree of head protraction. The CC angle was also measured using the Kinovea software (ver. 0.8.18, Kinovea open-source project, https://www.kinovea.org/) under the same conditions as the CV angle.
Both neck angles were analysed using the Kinovea software. Kinovea is widely used analysis software with excellent intra-rater (ICC = 0.99) and inter-rater (ICC = 0.99) reliability [15] and is consistently used for analysing head posture angles [16].
Statistical analysis
Data were presented using descriptive statistics, including mean, median, standard deviation, minimum, and maximum values. The normality of the data distribution was assessed using the Shapiro–Wilk test and Q-Q plots.
Linear mixed-effects models (LMM) were used to account for the repeated-measures design, where the same children were measured in both first and fifth grades. Separate LMMs were conducted for each dependent variable: sagittal and vertical CoG shifts, CV angle, and CC angle. Models were fitted using restricted maximum likelihood estimation (REML), and significance was tested using Satterthwaite’s method for estimating degrees of freedom. The significance level was set at p < 0.05. Model assumptions were assessed using standard diagnostic tests. Linearity and homo-scedasticity were evaluated by plotting residuals against fitted values. Normality of residuals was assessed with Q-Q plots and the Shapiro–Wilk test. Homoscedasticity was also tested with the Breusch–Pagan test and simulated residuals. The independence of the residuals was assessed using the Durbin–Watson test, and multicollinearity was evaluated using variance inflation factors (VIF).
For CoG shift, grade (first vs. fifth) and BMI were treated as fixed effects, and subject ID was treated as a random effect to account for within-subject variability. For neck angles, condition (no-bag vs. bag), grade (first vs. fifth), BMI, and their interaction terms were treated as fixed effects, while subject ID was once again included as a random effect with random intercept and slope.
Effect sizes were reported using estimated marginal means and standard errors. All analyses were performed in R, ver. 4.3.1. [17] using the lme4 [18], lmer-Test [19], lmtest [20], and DHARMa [21] packages.
Results
Table 1 presents the basic anthropometric characteristics of the sample in the first and fifth grades. On average and unsurprisingly, the children were taller and heavier in the fifth grade compared to the first grade. Males and females had similar average body weight and BMI in both grades. Schoolbag weight increased from first to fifth grade for both sexes, with females generally carrying slightly heavier bags. The percentage of schoolbag weight relative to body weight decreased from first to fifth grade, indicating that the increase in body weight outpaced the increase in schoolbag weight.
Table 1
Basic anthropometric characteristics of the sample (male = 28, female = 32)
Table 2 shows the basic kinematic characteristics of the sample in the first and fifth grades. On average, the sagittal CoG shift was higher in the males than in the females in both grades, with a slight increase from first to fifth grade for both sexes. The vertical CoG shift was larger in the first grade compared to the fifth grade, with males showing greater vertical shifts than females. Craniovertebral (CV) and craniocervical (CC) angles were generally higher in the females than in the males. The encumbered CV and CC angles were consistently lower than the unencumbered angles across both grades, with a slight increase from first to fifth grade. The variability in CoG shifts and angles was relatively low, as reflected by the small standard deviations.
Table 2
Basic kinematic characteristics of sample (male = 28, female = 32)
[i] 1 – 1st grade, 2 – 2nd grade, CoG – centre of gravity, CVA – craniovertebral angle, CCA – craniocervical angle A positive sagittal shift reflects forward CoG movement, while a negative value ref A positive vertical shift reflects inferior CoG movement, while a negative value reflects a posterior shift. lects a superior shift.
Table 3 shows the fixed effects of the LMM for sagittal CoG shift. The estimated effect of moving from first to fifth grade was a 0.46 cm forward shift, but this effect was not statistically significant (p = 0.139), suggesting that AP shift remains stable across grades. BMI was a significant predictor (p = 0.016), with each 1-unit increase in BMI linked to a 0.13 cm decrease in forward CoG shift, indicating that larger or heavier children tend to shift their CoG more to the posterior under load than their smaller or lighter peers. For the random effects, the within-child variation was small (0.025 cm), suggesting consistent postural responses within children across different grades.
Table 3
Linear mixed-effects model (CoG shift ~ grade + BMI)
| Predictor | Estimate (cm) | SE (cm) | t-value | p -value |
|---|---|---|---|---|
| Sagittal CoG shift | ||||
| (5th) | 0.46 | 0.31 | 1.49 | 0.139 |
| BMI | –0.13 | 0.05 | –2.45 | 0.016* |
| Vertical CoG shift | ||||
| grade (5th) | –0.36 | 0.10 | –3.66 | < 0.001* |
| BMI | –0.04 | 0.02 | –1.68 | 0.097 |
Table 3 also shows the fixed effects of the LMM for a vertical CoG shift. Moving from first to fifth grade was associated with a 0.36 cm upward shift, which was also statistically significant (p < 0.001), suggesting that older children have less of an inferior CoG shift when encumbered by a schoolbag. BMI had a marginal effect (p = 0.097), with each 1-unit increase in BMI linked to a 0.04 cm upward shift, suggesting that heavier children may experience slightly smaller downward shifts under load. For the random effects, the small intercept variance (0.0015 cm) and residual variance (0.0022 cm) indicate that a vertical CoG shift was consistent both between and within children.
Table 4 shows the fixed effect of the LMM for the craniovertebral angle (CV). Carrying a bag was associated with a significant 5.53° decrease in CV angle (p < 0.001), suggesting a more forward head position when carrying a load. The effect of grade was not significant (p = 0.211), with the CV angle increasing by only 1.13° from first to fifth grade. BMI was a significant predictor (p < 0.001), with each 1-unit increase in BMI linked to a 0.62° decrease in CV angle, indicating that heavier children tend to adopt a more forward head position. The interaction between grade and condition was not significant (p = 0.172), suggesting that the bag’s effect on CV angle did not differ by grade. For the random effects, the intercept variance (12.39°) and slope variance (0.03°) indicate moderate individual differences in baseline CV angle but very consistent responses to the bag condition across children.
Table 4
Linear mixed-effects model (neck angle ~ condition * grade + BMI)
Table 4 also shows the fixed effect of the LMM for the craniocervical angle (CC). Carrying a bag was associated with a significant 2.70° increase in the CC angle (p = 0.018). As with the CV angle, this also indicates a more protracted head posture when encumbered with a schoolbag. Moving from first to fifth grade showed a significant 2.99° increase in the CC angle (p = 0.017), indicating that the CC angle increases with age. BMI had a positive but non-significant effect on the CC angle (0.35° per unit increase in BMI, p = 0.205). The interaction between grade and condition was also not significant (p = 0.785), meaning that the school-bag’s effect on the CC angle likely did not differ between grades. Also, very similarly to the CV angles, the random intercept variance (33.28°) and random slope variance (0.32°) showed moderate individual differences in baseline CC angle but very consistent responses to the bag condition across children.
Discussion
The present study aimed to investigate how school-bag load affects posture and body mechanics in children across two key educational stages, first and fifth grade, through a combination of anthropometric and kinematic analyses. The intention was to evaluate how growing bodies respond to external load in terms of both biomechanical posture and stability.
As expected, children in fifth grade were significantly taller and heavier than their first-grade equivalents. Although the absolute weight of schoolbags increased with grade level, the relative load decreased: in first grade, schoolbags represented on average 15.1% of body weight in boys and 17.7% in girls, whereas in fifth grade this fell to 12.3% and 13.0%, respectively. Despite this proportional reduction, postural adaptations due to schoolbag carriage were still clearly observed in both age groups. This aligns with reports that deviations can occur even when schoolbag weight remains within the recommended 10–15% of body weight [22]. Our findings therefore suggest that physical maturation alone does not fully mitigate compensatory responses to external load.
The most pronounced postural change induced by the schoolbag was a reduction in CV angle and an increase in CC angle, indicating forward head posture. In our models, carrying a bag decreased the CV angle by 5.53° and increased the CC angle by 2.70°, demonstrating a consistent shift toward head protraction. These findings are broadly consistent with previous work showing cervical adaptations under load [23], and our longitudinal design shows that these compensations persist despite physical maturation. BMI emerged as a significant predictor of CV angle: children with higher BMI exhibited more pronounced forward head posture. This demonstrates the interplay between external load and body composition and is consistent with broader public health concerns regarding childhood obesity and its musculoskeletal consequences [24, 25]. Heavier children may rely on stronger compensatory strategies to stabilise the head and trunk under load.
CoG responses further illustrate these compensatory patterns. Sagittal CoG shift remained relatively stable across grades, whereas vertical CoG displacement decreased significantly with age by 0.36 cm, suggesting improved load-handling capacity as children grow. BMI was also a significant predictor of sagittal CoG shift: each 1-unit increase in BMI was associated with a 0.13 cm decrease in forward CoG displacement, indicating that larger or heavier children tended to shift their CoG less anteriorly under load than their lighter peers. By contrast, BMI was not significantly associated with vertical CoG movement, suggesting that body composition influenced how children controlled the fore-aft position of their CoG rather than its vertical displacement. However, even this improvement did not eliminate compensatory mechanisms, indicating that the neuromuscular system continues to adapt under load. Prior studies have linked repeated load carriage to altered sensory integration and changes in neuro-motor control [26], and our findings support this perspective by demonstrating persistent CoG adjustments in both younger and older children. Comparable associations between postural alignment and functional balance have been observed in athletic youth populations as well, such as in 10–12-year-old wrestlers, where posture was linked to dynamic balance performance [27]. Together, these findings underscore the importance of considering body composition and neuromotor control in understanding children’s postural adaptations to load.
These biomechanical observations underscore the importance of school-based ergonomic interventions. Previous research shows that posture education can improve backpack handling and spinal alignment [28, 29], and our findings reinforce the practical value of such programmes. Given the observed influence of BMI on cervical posture, preventive strategies may be particularly important for children with higher body mass, who appear more vulnerable to load-related deviations. Although our study captures medium-term adaptations, the potential long-term consequences of habitual forward head posture and altered CoG control warrant further exploration. Future studies should integrate balance assessments or proprioceptive testing to better understand how load carriage interacts with neuromuscular development over time.
Study limitations
Several limitations of this study should be acknowledged. First, although our four-year follow-up captures short- to medium-term adaptations, it does not allow us to determine whether the observed compensations accumulate into long-term musculoskeletal problems; longer prospective studies with repeated biomechanical and clinical assessments will be needed to address this.
Second, all postural measurements were obtained in a static standing condition, which does not fully reflect natural posture dynamics during walking or everyday school activities, so our findings should be interpreted as a snapshot of quiet standing rather than dynamic function. Third, although anthropometric data were reported separately for boys and girls, sex-related differences were not modelled in the linear mixed-effects analyses; given potential differences in maturation rate and body composition, future studies with larger samples should explicitly examine sex-specific effects and their interactions with schoolbag load and BMI.
Conclusions
The results of this longitudinal study indicate that postural adaptations, particularly in the head and neck region, do occur over a four-year period in school-aged children, with measurable changes in craniocervical and craniovertebral angles. While these changes suggest a compensatory response to mechanical load, the extent of the postural deviation observed was relatively moderate. The data also showed an increase in school-bag weight over time and a persistently high ratio of bag weight to body weight, especially among younger students. The lack of standardised procedures and variability in individual development further complicate the interpretation of the results. Therefore, ongoing monitoring and the implementation of preventive measures in schools remain important steps in supporting healthy postural development.
In practical terms, these findings highlight the importance of monitoring backpack weight and promoting healthy load-carrying habits in everyday school life. Teachers and parents can help by encouraging children to wear both shoulder straps, adjust backpack height so that it rests close to the trunk, and regularly review the contents to avoid unnecessary weight. Children with higher BMI might require particular attention, as they appear more vulnerable to load-related postural deviations. Healthcare professionals and school-based physiotherapists can support these efforts through brief posture-education sessions and routine screening of children who report discomfort. Implementing these simple, low-cost strategies may help reduce compensatory postural patterns and support healthier musculoskeletal development during key growth stages.